
Skin Cancer
There are a few types of skin cancers. Over here at this page we will discuss about Basal Cell Carcinoma, Bowen Disease, Keratoacanthoma, Melanoma and Squamous Cell Carcinoma.
Basal cell Carcinoma
Basal cell carcinoma is also called BCC, Basalioma or rodent ulcer. It is the commonest skin cancer. It tends to occur more commonly among fair-skinned individuals with repeated ultraviolet sun exposure, radiation exposure and sunburns. The estimated lifetime risk for BCC in the white population is 33-39% for men and 23-28% for women.
There are a few types of skin cancers. Over here at this page we will discuss about Basal Cell Carcinoma, Bowen Disease, Keratoacanthoma, Melanoma and Squamous Cell Carcinoma.
Basal cell Carcinoma
Basal cell carcinoma is also called BCC, Basalioma or rodent ulcer. It is the commonest skin cancer. It tends to occur more commonly among fair-skinned individuals with repeated ultraviolet sun exposure, radiation exposure and sunburns. The estimated lifetime risk for BCC in the white population is 33-39% for men and 23-28% for women.
There may be certain genetic predisposition to develop BCC in families with basal cell nevus syndrome (Gorlin syndrome) or Bazex syndrome.
BCC is a non-melanocytic skin cancer that arises from basal cells that are small, round cells found in the lower layer of the epidermis. BCC rarely spreads to lymph nodes and distant organs hence its prognosis is usually good.
BCC is a non-melanocytic skin cancer that arises from basal cells that are small, round cells found in the lower layer of the epidermis. BCC rarely spreads to lymph nodes and distant organs hence its prognosis is usually good.
Clinical types of BCC
BCC tend to grow slowly over months to years, varying in sizes. Patient often presents with a lesion that enlarges with time, does not heal and sometimes bleed when sometimes traumatized. More than 80% of BCC occur over at the head and neck region especially on the nose.
BCC tend to grow slowly over months to years, varying in sizes. Patient often presents with a lesion that enlarges with time, does not heal and sometimes bleed when sometimes traumatized. More than 80% of BCC occur over at the head and neck region especially on the nose.
There are a few types of BCC:
1.Nodular BCC: This is the most common form of BCC found usually on the face. Sometimes they may occur on the trunk and extremities. They appear as pearly flesh-colored to pinkish lump with blood vessels on its surface (telangiectasia). When it grows, it forms a center ulcer with rolled up edges. It tends to bleed easily. It may be mistaken as a cyst.
1.Nodular BCC: This is the most common form of BCC found usually on the face. Sometimes they may occur on the trunk and extremities. They appear as pearly flesh-colored to pinkish lump with blood vessels on its surface (telangiectasia). When it grows, it forms a center ulcer with rolled up edges. It tends to bleed easily. It may be mistaken as a cyst.
2.Cystic BCC: it is an uncommon variant of nodular BCC. It appears as a bluish-grey cystic lesion filled with jellylike clear mucin in the center.
3.Pigmented BCC: It is more common in Asians and less common in Caucasians. The lesion can be blue, brown or gray in color. It may be difficult to differentiate them from melanoma.
4.Morpheaform (sclerosing) BCC: It is an uncommon variant whereby the tumor cells induce fibroblasts and collagen deposition (sclerosis) resulting in a scar-like lesion. It appears as a white-yellow waxy scar like lesion that if spread will spread through the cutaneous nerves. It seldom ulcerates and bleeds. It is more common in Caucasians.
5.Superficial BCC: It is more commonly found on the shoulders and trunks and in younger patients. There may be multiple pink/red scaly well-circumscribed patches with a whitish scale. Minute eschars may appear within the patch. It grows slowly hence it is less likely to turn invasive form of cancer.
6.Infiltrative Basal Cell Carcinoma: the cancer infiltrates the dermis in between the collagen fibers making the cancer margin difficult to determine. It has higher recurrence rate compared with nodular BCC.
7.Micronodular Basal Cell Carcinoma: this is the aggressive subtype of BCC which appears yellow-white when stretched. It does not ulcerate easily and is firm to touch. It usually has well-defined margins.
Diagnosis of basal cell carcinoma
As BCC rarely metastasize (spread), laboratory and imaging studies are seldom indicated. Unless there is suggestion of spread to deeper structures e.g. bones the imaging studies (e.g. CT scan) may be necessary.
Skin biopsy is usually done to confirm the diagnosis and also to determine the subtype of BCC.
As BCC rarely metastasize (spread), laboratory and imaging studies are seldom indicated. Unless there is suggestion of spread to deeper structures e.g. bones the imaging studies (e.g. CT scan) may be necessary.
Skin biopsy is usually done to confirm the diagnosis and also to determine the subtype of BCC.
Staging of BCC
Stage 0: Cancer involves only the epidermis and has not spread to the dermis.
Stage I: Cancer is less than 2 cm and has not spread to the lymph nodes or other organs
Stage II: Cancer is more than 2 cm but has not spread to lymph nodes or other organs
Stage III: Cancer has spread to tissues beneath the skin (e.g., muscle,
bone, cartilage), and/or to regional lymph nodes but not to other organs.
Stage IV: Cancer can be any size and has spread to other organs.
Treatment of BCC
Treatment modality depends on the type of BCC, its size, location, stage of disease and also patients’ preference. Treatment modalities include topical treatment, surgical treatment, photodynamic therapy, radiation therapy and systemic chemotherapy (for advance disease that has spread to other organs).
Topical treatment
Low risk patients with small superficial BCC that is non-recurring can opt for topical treatment with creams.
1.Topical 5-fluorouracil 5% cream: It can be used for very superficial small BCC. It interferes with DNA synthesis and, subsequently reduces cell proliferation. It should be applied twice daily for at least 6 weeks. Irritation and crusting are common side effects.
2.Imiquinod 5% cream (Aldara): It is an immune response modifier used for small BCC of less than 1 cm. Treatment is usually initiated at 3 times per week and is increased as tolerated to once daily, and even twice daily if tolerated for about 6-12 weeks. It may cause skin irritation. Cure rate is about 70-80%.
Stage 0: Cancer involves only the epidermis and has not spread to the dermis.
Stage I: Cancer is less than 2 cm and has not spread to the lymph nodes or other organs
Stage II: Cancer is more than 2 cm but has not spread to lymph nodes or other organs
Stage III: Cancer has spread to tissues beneath the skin (e.g., muscle,
bone, cartilage), and/or to regional lymph nodes but not to other organs.
Stage IV: Cancer can be any size and has spread to other organs.
Treatment of BCC
Treatment modality depends on the type of BCC, its size, location, stage of disease and also patients’ preference. Treatment modalities include topical treatment, surgical treatment, photodynamic therapy, radiation therapy and systemic chemotherapy (for advance disease that has spread to other organs).
Topical treatment
Low risk patients with small superficial BCC that is non-recurring can opt for topical treatment with creams.
1.Topical 5-fluorouracil 5% cream: It can be used for very superficial small BCC. It interferes with DNA synthesis and, subsequently reduces cell proliferation. It should be applied twice daily for at least 6 weeks. Irritation and crusting are common side effects.
2.Imiquinod 5% cream (Aldara): It is an immune response modifier used for small BCC of less than 1 cm. Treatment is usually initiated at 3 times per week and is increased as tolerated to once daily, and even twice daily if tolerated for about 6-12 weeks. It may cause skin irritation. Cure rate is about 70-80%.
3. Tazarotene is a retinoid that cause BCC regression by increasing apoptosis and by decreasing cell proliferation in the skin cancer cells. It is used to treat small low risks BCC and has to be used for 5-8 months. It may cause skin dryness and irritation.
Surgical Therapy
It involves surgical removal of the cancer with the best possible
cosmetic result.
1.Cryotherapy: using liquid nitrogen to freeze the superficial BCC. Subsequently a blister forms followed by crusting and healing in weeks. It may leave a permanent white scar.
It involves surgical removal of the cancer with the best possible
cosmetic result.
1.Cryotherapy: using liquid nitrogen to freeze the superficial BCC. Subsequently a blister forms followed by crusting and healing in weeks. It may leave a permanent white scar.
2.Minor surgery: Like shave biopsy, curettage & cautery can be used to remove small superficial or nodular BCC. The wound will heal within weeks.
3.Excision biopsy: It is appropriate treatment nodular, infiltrative and morphoeic BCCs. The cancer is cut out surgically with about 3-4 mm of additional normal skin margin and then the wound is stitched up. If the cancer is large then a skin graft or flap may be necessary to close the defect post excision of cancer. If the cancer is inadequately removed or if it recurs, further surgery may be necessary.
4. Mohs micrographically controlled excision is a technique used for BCCs over at high-risk areas of the face around the eyes, nose and lips, ill-defined BCCs (any subtype), morphoeic BCCs and recurrent BCC. It involves examining excised tissue under the microscope carefully layer by layer while patient is still in the operating theatre. Several slices may need to be excised until the cancer has been completely removed.
Photodynamic therapy
A photosensitizing cream (e.g. Metvix or ALA) is applied over the lesion and then exposed to certain wavelengths of light. The side effects include local edema (swelling), erythema (redness), blistering, and ulceration. The cure rate is about 53% for superficial BCC and 83% for Nodular BCC. It has good cosmetic result.
A photosensitizing cream (e.g. Metvix or ALA) is applied over the lesion and then exposed to certain wavelengths of light. The side effects include local edema (swelling), erythema (redness), blistering, and ulceration. The cure rate is about 53% for superficial BCC and 83% for Nodular BCC. It has good cosmetic result.
Radiation therapy
Radiation therapy using radiation to treat BCC is used for extended and advance lesions and for patients who are not suitable to undergo surgery. Repeated sections may be required and it is more expensive. Cosmetic effect is good.
Radiation therapy using radiation to treat BCC is used for extended and advance lesions and for patients who are not suitable to undergo surgery. Repeated sections may be required and it is more expensive. Cosmetic effect is good.
Hedgehog Pathway Inhibitors
Vismodegib is FDA approved drug since March 2012. It selectively inhibits Smoothened (SMO) which is a key protein involved in hedgehog signal transduction of cancerous cells. It is usually reserved for patients with advanced or metastasized (spread to other organs) BCC.
Vismodegib is FDA approved drug since March 2012. It selectively inhibits Smoothened (SMO) which is a key protein involved in hedgehog signal transduction of cancerous cells. It is usually reserved for patients with advanced or metastasized (spread to other organs) BCC.
What is Bowen Disease?
Bowen disease is also known as intraepidermal squamous cell carcinoma or cutaneous squamous cell carcinoma in situ. ‘In situ’ means the cancer cells are confined to cell of origin which is the epidermis. The cancer involves the squamous cells, the flat cells that make up the outset layer of the skin called the epidermis. The risk of progression to invasive Squamous Cell Carcinoma is about 3-5%. The risk is higher if Bowen disease involves the genital area.
Bowen disease is a common type of skin cancer. It is more common in the sun-exposed areas of fair-skinned people. The highest incidence occurs in the elderly group above 60 years old. There is no gender preference.
Bowen disease is also known as intraepidermal squamous cell carcinoma or cutaneous squamous cell carcinoma in situ. ‘In situ’ means the cancer cells are confined to cell of origin which is the epidermis. The cancer involves the squamous cells, the flat cells that make up the outset layer of the skin called the epidermis. The risk of progression to invasive Squamous Cell Carcinoma is about 3-5%. The risk is higher if Bowen disease involves the genital area.
Bowen disease is a common type of skin cancer. It is more common in the sun-exposed areas of fair-skinned people. The highest incidence occurs in the elderly group above 60 years old. There is no gender preference.
Causes of Bowen Disease
Bowen disease is caused by a variety of factors which include:
1.Long term UV exposure: Bowen disease happens on sun-exposed areas in elderly patients which suggest that chronic sun exposure is a factor that causes the cancer. In fact UV radiation damages the skin cell DNA resulting in gene p53 mutation and uncontrolled growth of the skin cells. UV radiation also suppresses the immune response preventing recovery from this damage.
2.Human Papillomavirus (HPV): Type 16 has been associated with Bowen disease involving the genital area.
Bowen disease is caused by a variety of factors which include:
1.Long term UV exposure: Bowen disease happens on sun-exposed areas in elderly patients which suggest that chronic sun exposure is a factor that causes the cancer. In fact UV radiation damages the skin cell DNA resulting in gene p53 mutation and uncontrolled growth of the skin cells. UV radiation also suppresses the immune response preventing recovery from this damage.
2.Human Papillomavirus (HPV): Type 16 has been associated with Bowen disease involving the genital area.
3.Arsenic exposure: after several years of exposure, Bowen disease may occur on the trunks and limbs area.
4.Immunosupressed patients: may have more aggressive and advanced Bowen disease.
5.Other factors: Genetic factors, cancer-causing chemicals, radiation and trauma may predispose one to Bowen disease.
Clinical presentation of Bowen Disease
Patients usually present with a red, well demarcated scaly patch which does not cause much symptoms. The lesion usually tends to grow slowly and is found mainly on sun exposed skin surfaces like the head, neck, ears, hands and limbs areas. The size can vary from several millimeters to few centimeters in diameter. The lesion can become crusted, ulcerates, thicken (hyperkeratotic) and fissured. The lesion seldom gets pigmented.
4.Immunosupressed patients: may have more aggressive and advanced Bowen disease.
5.Other factors: Genetic factors, cancer-causing chemicals, radiation and trauma may predispose one to Bowen disease.
Clinical presentation of Bowen Disease
Patients usually present with a red, well demarcated scaly patch which does not cause much symptoms. The lesion usually tends to grow slowly and is found mainly on sun exposed skin surfaces like the head, neck, ears, hands and limbs areas. The size can vary from several millimeters to few centimeters in diameter. The lesion can become crusted, ulcerates, thicken (hyperkeratotic) and fissured. The lesion seldom gets pigmented.
Diagnosis of Bowen Disease
A skin biopsy is often done to confirm the diagnosis of Bowen disease.
A skin biopsy is often done to confirm the diagnosis of Bowen disease.
Treatment of Bowen Disease
There are several treatment modalities available. The treatment of choice depends on whether patient is immunosuppressed, if there are multiple lesions, any history of recurrences and whether lesions are found on high-risk areas. As there may be a tendency of recurrence, patients should be followed up for 6-12 months post treatment.
The forms of treatment include topical treatment, photodynamic therapy, radiation therapy and surgical excision. They will be described below:
Topical treatment
1.Topical 5-fluorouracil 5% cream: It interferes with DNA synthesis and, subsequently reduces cell proliferation. It should be applied once to twice daily for 4 to 12 weeks. Irritation and crusting are common side effects.
There are several treatment modalities available. The treatment of choice depends on whether patient is immunosuppressed, if there are multiple lesions, any history of recurrences and whether lesions are found on high-risk areas. As there may be a tendency of recurrence, patients should be followed up for 6-12 months post treatment.
The forms of treatment include topical treatment, photodynamic therapy, radiation therapy and surgical excision. They will be described below:
Topical treatment
1.Topical 5-fluorouracil 5% cream: It interferes with DNA synthesis and, subsequently reduces cell proliferation. It should be applied once to twice daily for 4 to 12 weeks. Irritation and crusting are common side effects.
2. Imiquinod 5% cream (Aldara): It is an immune response modifier used successfully for Bowen disease which involves larger lesions. It should be applied five times weekly for six to sixteen weeks. It may cause skin irritation.
Photodynamic therapy
A photosensitizing cream (e.g. Metvix or ALA) is applied over the lesion and then exposed to certain wavelengths of light. The side effects include local edema (swelling), erythema (redness), burning, stinging, skin discoloration, blistering, and ulceration. The cure rate appears to be good.
A photosensitizing cream (e.g. Metvix or ALA) is applied over the lesion and then exposed to certain wavelengths of light. The side effects include local edema (swelling), erythema (redness), burning, stinging, skin discoloration, blistering, and ulceration. The cure rate appears to be good.
Radiation therapy
Radiation therapy using radiation to treat Bowen is used for extended and advance multiple lesions and for patients who are not suitable to undergo surgery. Repeated sections may be required and it is more expensive. Cosmetic effect is good.
Radiation therapy using radiation to treat Bowen is used for extended and advance multiple lesions and for patients who are not suitable to undergo surgery. Repeated sections may be required and it is more expensive. Cosmetic effect is good.
Surgical Therapy
It involves surgical removal of the cancer with the best possible cosmetic result.
1.Cryotherapy: using liquid nitrogen to freeze the small patches of Bowen disease lesions. A blister forms after freezing followed by crusting and healing in weeks. It may leave a permanent white scar. There may be risk of poor healing.
It involves surgical removal of the cancer with the best possible cosmetic result.
1.Cryotherapy: using liquid nitrogen to freeze the small patches of Bowen disease lesions. A blister forms after freezing followed by crusting and healing in weeks. It may leave a permanent white scar. There may be risk of poor healing.
2.Minor surgery: Like shave biopsy, curettage & cautery can be used to remove small superficial Bowen disease. The wound will heal within weeks. It may not be as effective as Mohs micrographically controlled excision.
3.Excision biopsy: It is most common and appropriate treatment for smaller lesions not involving the face and digits. The cancer is cut out surgically with about 4 mm of additional normal skin margin and then the wound is stitched up. If the cancer is large then a skin graft or flap may be necessary to close the defect post excision of cancer. If the cancer is inadequately removed or if it recurs, further surgery may be necessary.
4. Mohs micrographically controlled excision is a technique used for larger poorly demarcated lesions, recurrent lesions on the head and neck or on areas where tissue sparing is vital like the digits and genital area. It involves examining excised tissue under the microscope carefully layer by layer while patient is still in the operating theatre. Several slices may need to be excised until the cancer has been completely removed.
What is Keratoacanthoma?
Keratoacanthoma is a low grade tumor that originates in pilosebaceous glands and resembles squamous cell carcinoma. It is a skin lesion that erupts over sun-damaged/hair-bearing skin area. It grows rapidly over few weeks to months followed by spontaneous resolution over the next 4 to 6 months.
Keratoacanthoma is less frequent among dark-skinned people. Male to female ratio is about 2:1. It can occur at any age but more common as one age.
Keratoacanthoma is a low grade tumor that originates in pilosebaceous glands and resembles squamous cell carcinoma. It is a skin lesion that erupts over sun-damaged/hair-bearing skin area. It grows rapidly over few weeks to months followed by spontaneous resolution over the next 4 to 6 months.
Keratoacanthoma is less frequent among dark-skinned people. Male to female ratio is about 2:1. It can occur at any age but more common as one age.
What causes Keratoacanthoma?
The exact etiology for formation of Keratoacanthoma remains unknown. Sunlight, chemical carcinogens, trauma/injury, HPV virus, genetic factors and immunocompromised state may predispose one to form Keratoacanthoma.
The exact etiology for formation of Keratoacanthoma remains unknown. Sunlight, chemical carcinogens, trauma/injury, HPV virus, genetic factors and immunocompromised state may predispose one to form Keratoacanthoma.
Clinical presentation
Keratoacanthoma often occur at sun exposed areas like the face, neck and the upper limbs. They are usually single lesions that begin as round, firm, skin-colored/reddish papules that will progress to dome-shaped nodules with smooth surface but with a central ulcer or keratin plug which may grow into a horn.
Keratoacanthoma often occur at sun exposed areas like the face, neck and the upper limbs. They are usually single lesions that begin as round, firm, skin-colored/reddish papules that will progress to dome-shaped nodules with smooth surface but with a central ulcer or keratin plug which may grow into a horn.
Treatment of Keratoacanthoma
As Keratoacanthoma resembles squamous cell carcinoma hence excision biopsy and histopathology confirmation of the lesion is warranted for diagnosis.
As Keratoacanthoma resembles squamous cell carcinoma hence excision biopsy and histopathology confirmation of the lesion is warranted for diagnosis.
Keratoacanthoma can be removed surgically by excision, cryotherapy, curettage & cautery and also by radiotherapy. For patients who are poor surgical candidates, then intra-lesional methotrexate (MTX), [22] 5-fluorouracil, bleomycin, and steroids can be used.
What is melanoma?
Melanoma is a serious skin cancer which results from uncontrolled growth of skin pigment cells (melanocytes). Melanocytes are found in the basal layer of the epidermis. The melanocytes produce a protein skin pigment called melanin, which absorbs the ultraviolet (UV) radiation and protects the skin. Darker-skinned individuals produce more melanin.
Melanoma is a serious skin cancer which results from uncontrolled growth of skin pigment cells (melanocytes). Melanocytes are found in the basal layer of the epidermis. The melanocytes produce a protein skin pigment called melanin, which absorbs the ultraviolet (UV) radiation and protects the skin. Darker-skinned individuals produce more melanin.
Non-cancerous growth of melanocytes present as moles (melanocytic naevi) and freckles (ephelides and lentigines). Cancerous growth of melanocytes forms melanoma.
Queensland, Australia, has the highest incidence of melanoma in the world. Fairer skinned people are more likely to get melanoma compared with darker skinned people. It is slightly more common in men than women. The age onset can occur at any age, average age of diagnosis is 57.
Queensland, Australia, has the highest incidence of melanoma in the world. Fairer skinned people are more likely to get melanoma compared with darker skinned people. It is slightly more common in men than women. The age onset can occur at any age, average age of diagnosis is 57.
Types of melanoma
Melanoma has 3 growth phases mainly radial and vertical phases. In radial phase, the cancerous cells grow in a radial horizontal fashion in the epidermis (outermost layer of skin). As melanomas progresses and grows in time into the vertical growth phase, the cancer cells invade the dermis (deeper layer of skin) and spread to distant organs via the bloodstream and lymphatic drainage.
There are 5 different histologic types of melanoma include Superficial spreading melanomas, Nodular melanomas, Lentigo maligna melanomas, Acral lentiginous melanomas and Mucosal lentiginous melanomas.
Melanoma has 3 growth phases mainly radial and vertical phases. In radial phase, the cancerous cells grow in a radial horizontal fashion in the epidermis (outermost layer of skin). As melanomas progresses and grows in time into the vertical growth phase, the cancer cells invade the dermis (deeper layer of skin) and spread to distant organs via the bloodstream and lymphatic drainage.
There are 5 different histologic types of melanoma include Superficial spreading melanomas, Nodular melanomas, Lentigo maligna melanomas, Acral lentiginous melanomas and Mucosal lentiginous melanomas.
Staging and prognosis of melanoma
Melanoma being a cancer has a staging system like other cancers to determine the stage of the cancer. The few staging systems are described below.
TNM Classification of Melanoma
Melanoma being a cancer has a staging system like other cancers to determine the stage of the cancer. The few staging systems are described below.
TNM Classification of Melanoma
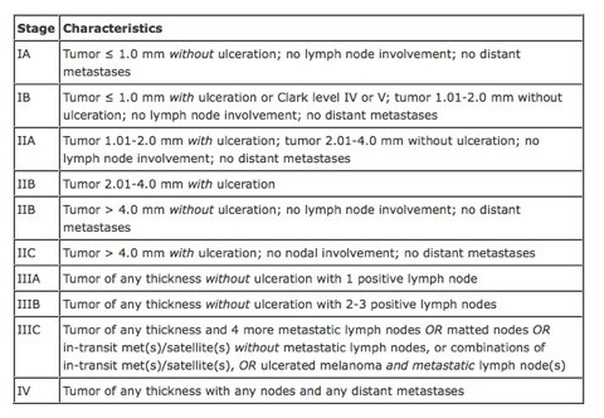
American Joint Committee on Cancer (AJCC) on Melanoma
Clark staging:
Level I - All tumor cells above basement membrane (in situ)
Level II - Tumor extends into papillary dermis
Level III - Tumor extends to interface between papillary and reticular dermis
Level IV - Tumor extends between bundles of collagen of reticular dermis (extends into reticular dermis)
Level V - Tumor invasion of subcutaneous tissue
Level I - All tumor cells above basement membrane (in situ)
Level II - Tumor extends into papillary dermis
Level III - Tumor extends to interface between papillary and reticular dermis
Level IV - Tumor extends between bundles of collagen of reticular dermis (extends into reticular dermis)
Level V - Tumor invasion of subcutaneous tissue
Prognosis of disease depends on the stage of disease, the presence or absence of ulceration, age of patient, the depth of invasion, the presence of lymph nodes, if spread to other organs is present at diagnosis.
Patents with stage I disease has a 5-year survival rate of greater than 90%.
Patients with stage II disease has a 5-year survival rate ranging from 45-77%.
Patients with stage III disease has a 5-year survival rate ranging from 27-70%.
Patients with metastatic disease (cancer that has spread to other organs) have a poor prognosis with a 5-year survival rate of less than 20%.
Risk factors for melanoma (cancerous moles)
1.Number of acquired moles: If patients have > 100 moles or Caucasians with > 40 moles by age 50, there is an increased risk of having a cancerous mole.
2.Dysplastic Nevi as discussed earlier is sometimes pre-cancerous moles.
Patents with stage I disease has a 5-year survival rate of greater than 90%.
Patients with stage II disease has a 5-year survival rate ranging from 45-77%.
Patients with stage III disease has a 5-year survival rate ranging from 27-70%.
Patients with metastatic disease (cancer that has spread to other organs) have a poor prognosis with a 5-year survival rate of less than 20%.
Risk factors for melanoma (cancerous moles)
1.Number of acquired moles: If patients have > 100 moles or Caucasians with > 40 moles by age 50, there is an increased risk of having a cancerous mole.
2.Dysplastic Nevi as discussed earlier is sometimes pre-cancerous moles.
3.Personal history of melanoma is also a risk factor.
4.Prolonged and excessive sun exposure as well as severe sunburns predispose to cancerous moles. Ultraviolet A with wavelength 320-400 nm and ultraviolet B with wavelength 290-320 nm are cancer inducing ultraviolet radiation. The UV radiation suppresses the immune system of the skin, induce melanocyte cell division, damage of melanocyte DNA and free radical production resulting in cancer cells formation.
5.Large congenital nevi larger than 20 cm has increased risk of melanoma.
6.Certain genes like CDKN2A (p16), CDK4, RB1, CDKN2A (p19), PTEN/MMAC1, and ras may predispose one to melanoma.
7.Immunosupressed individuals may also have higher risk of developing melanoma.
Clinical history taking for melanoma
The dermatologists will often take a clinical history and ask the patient few questions before examination to determine the risk factors.
Important questions to be asked include:
1.Family history of melanoma
2.Personal history of melanoma
3.Any prolonged sun exposure or previous serious sunburns
4.Moles: any change in size, color, shape, symmetry or new symptoms like itch, bleeding, ulceration.
5.Systemic review to rule out spread of melanoma to other organs:
-General: loss of weight loss & appetite, weakness, fatigue, and unexplained fever
-Respiratory: Cough, bloody sputum, pneumonia, chest pain and shortness of breath
-Liver: Right upper abdominal pain with radiation to scapula on inspiration and jaundice
-Skin/Lymphatic: non-healing/bleeding skin lesions, bruises and color changes
- Gastrointestinal: Abdominal pain, bleeding, nausea, vomiting, poor appetite and constipation
-Musculoskeletal: Joint and Bone pain
-Neurological: Headache, visual disturbance, memory impairment, seizure, balance problems, local weakness, numbness, paralysis, blackouts, depression and mood changes.
Clinical presentation of melanoma
Features of melanoma
Certain features distinguish a melanoma from a normal mole. If the mole changes in shape, size, color and if patient has symptoms of itch or bleeds then the patient should seek a dermatologist advice.
The appearance of a mole suspicious of a cancerous melanoma can be remembered by mnemonic ABCDE. The suspicious cancerous melanoma will be Asymmetric, Borders of mole are irregular, Color is variegated, Diameter (increases in size) and Erosion/elevation (ulcer forms).
4.Prolonged and excessive sun exposure as well as severe sunburns predispose to cancerous moles. Ultraviolet A with wavelength 320-400 nm and ultraviolet B with wavelength 290-320 nm are cancer inducing ultraviolet radiation. The UV radiation suppresses the immune system of the skin, induce melanocyte cell division, damage of melanocyte DNA and free radical production resulting in cancer cells formation.
5.Large congenital nevi larger than 20 cm has increased risk of melanoma.
6.Certain genes like CDKN2A (p16), CDK4, RB1, CDKN2A (p19), PTEN/MMAC1, and ras may predispose one to melanoma.
7.Immunosupressed individuals may also have higher risk of developing melanoma.
Clinical history taking for melanoma
The dermatologists will often take a clinical history and ask the patient few questions before examination to determine the risk factors.
Important questions to be asked include:
1.Family history of melanoma
2.Personal history of melanoma
3.Any prolonged sun exposure or previous serious sunburns
4.Moles: any change in size, color, shape, symmetry or new symptoms like itch, bleeding, ulceration.
5.Systemic review to rule out spread of melanoma to other organs:
-General: loss of weight loss & appetite, weakness, fatigue, and unexplained fever
-Respiratory: Cough, bloody sputum, pneumonia, chest pain and shortness of breath
-Liver: Right upper abdominal pain with radiation to scapula on inspiration and jaundice
-Skin/Lymphatic: non-healing/bleeding skin lesions, bruises and color changes
- Gastrointestinal: Abdominal pain, bleeding, nausea, vomiting, poor appetite and constipation
-Musculoskeletal: Joint and Bone pain
-Neurological: Headache, visual disturbance, memory impairment, seizure, balance problems, local weakness, numbness, paralysis, blackouts, depression and mood changes.
Clinical presentation of melanoma
Features of melanoma
Certain features distinguish a melanoma from a normal mole. If the mole changes in shape, size, color and if patient has symptoms of itch or bleeds then the patient should seek a dermatologist advice.
The appearance of a mole suspicious of a cancerous melanoma can be remembered by mnemonic ABCDE. The suspicious cancerous melanoma will be Asymmetric, Borders of mole are irregular, Color is variegated, Diameter (increases in size) and Erosion/elevation (ulcer forms).
Mole suspicious of melanoma should be measured for its thickness, size and location. Thorough examination for other moles should also be conducted. Lymph nodes should be palpated to rule out any spread to the lymphatic system.
Investigation for melanoma
1.Dermoscopy: examination may help the clinician identify the features of melanoma
Investigation for melanoma
1.Dermoscopy: examination may help the clinician identify the features of melanoma
2. Biopsy for histopathology examination: Full thickness biopsy is the standard diagnostic approach to look for invasion and margins of melanoma. Before biopsy, photographic documentation of the lesion is strongly recommended.
The Breslow thickness is measured vertically in millimeters from the top of the granular layer to the deepest point of tumor involvement. It is a strong predictor of outcome; the thicker the melanoma, the more likely it is to metastasize (spread to other organs).
The Breslow thickness is measured vertically in millimeters from the top of the granular layer to the deepest point of tumor involvement. It is a strong predictor of outcome; the thicker the melanoma, the more likely it is to metastasize (spread to other organs).
3.Blood tests: Full blood count, LDH, Liver enzymes may be measured if melanoma is suspected to have spread to other organs.
4.Lymph node biopsy: Any involved lymph nodes should be dissected. The sentinel lymph node is the first lymph node that the cancer cells will spread to should be biopsied to test if positive for cancer cells.
5.Imaging: Chest X-ray can be done to look for spread to lungs. Other scans like CT, MRI and PET may be necessary if the cancer is advance and have spread to other organs.
4.Lymph node biopsy: Any involved lymph nodes should be dissected. The sentinel lymph node is the first lymph node that the cancer cells will spread to should be biopsied to test if positive for cancer cells.
5.Imaging: Chest X-ray can be done to look for spread to lungs. Other scans like CT, MRI and PET may be necessary if the cancer is advance and have spread to other organs.
Treatment of melanoma
Surgery is the mainstay treatment for early stages of melanoma. Wide local excision with adequate margins plus sentinel lymph node biopsy and/or elective lymph node dissection is the mainstay of treatment for patients with primary melanoma.
Surgery is the mainstay treatment for early stages of melanoma. Wide local excision with adequate margins plus sentinel lymph node biopsy and/or elective lymph node dissection is the mainstay of treatment for patients with primary melanoma.
For advanced stages of melanoma, chemotherapy, radiotherapy and adjuncts (interferon and interleukins) may be used for treatment. Recurrence of disease is defined as regrowth of cancer within 2 cm from the surgical excision site. Treatment of choice involves wide excision of isolated local recurrences plus/minus adjuvant high dose interferon.
All melanoma patients post-surgery should be followed up regularly to examine the skin for recurrence and presence of lymph nodes. Blood tests and repeated scans may be done for more advanced cancer.
To prevent development of melanoma, one should reduce prolonged sun exposure and use sun screens with SPF of at least 15.
What is squamous cell carcinoma?
Squamous cell carcinoma, SCC, is the second commonest skin cancer after BCC. It accounts for 90% of head and neck cancers and 20% of skin cancers. It is derived from squamous cells that make up the outside layers of the skin (epidermis). These cells are keratinizing cells that produce keratin, a protein that makes up skin, hair and nails. It is more invasive compared with other skin cancers. It can spread to the nerves, blood stream to distant organs and through lymphatic drainage.
All melanoma patients post-surgery should be followed up regularly to examine the skin for recurrence and presence of lymph nodes. Blood tests and repeated scans may be done for more advanced cancer.
To prevent development of melanoma, one should reduce prolonged sun exposure and use sun screens with SPF of at least 15.
What is squamous cell carcinoma?
Squamous cell carcinoma, SCC, is the second commonest skin cancer after BCC. It accounts for 90% of head and neck cancers and 20% of skin cancers. It is derived from squamous cells that make up the outside layers of the skin (epidermis). These cells are keratinizing cells that produce keratin, a protein that makes up skin, hair and nails. It is more invasive compared with other skin cancers. It can spread to the nerves, blood stream to distant organs and through lymphatic drainage.
People living close to the equator present at a younger age than people living more distant from the equator. The highest incidence is in Australia. Fairer skinned and prolonged sun UV exposure are risk factors for SCC. Prevalence in men is about 2-3 times higher than women. The average age of presentation of SCC is about 70 years old.
What causes SCC?
SCC is caused by a combination of factors leading to cancerous changes in the squamous cells. The predisposing risk factors include:
1.UV radiation: Prolonged accumulative UV radiation exposure especially UVB (wavelength 290-320 nm) is one important factor that causes DNA damage and leading to SCC. PUVA phototherapy treatment in certain skin conditions like psoriasis also predispose one to SCC if done repeatedly at high doses. Indoor sun-tanning may also increase the risk of skin cancer.
What causes SCC?
SCC is caused by a combination of factors leading to cancerous changes in the squamous cells. The predisposing risk factors include:
1.UV radiation: Prolonged accumulative UV radiation exposure especially UVB (wavelength 290-320 nm) is one important factor that causes DNA damage and leading to SCC. PUVA phototherapy treatment in certain skin conditions like psoriasis also predispose one to SCC if done repeatedly at high doses. Indoor sun-tanning may also increase the risk of skin cancer.
2.Fair complexion: People who are fairer-skinned, those who havealbinism and those who get sunburn easily are at higher risk of developing SCC.
3.DNA defect: people with xeroderma pigmentosum have a deficiency in an enzyme which is needed for normal DNA repair and are more prone to of the develop SCC.
4.Immunosupression: Patients with HIV/AIDS, cancers (like lymphoproliferative conditions) and those taking immunosuppressing drugs e.g. organ transplant patients are at risk of developing SCC.
5.Smoking: tobacco usage has been associated with increased risk of most cancers especially head and neck SCC.
6.Alcohol: Drinking excessively is associated with increased risk of SCC head and neck just like smoking.
7.Age: with increasing age, there is increased risk of cancers in general.
8.Familial associated inherited conditions: Certain inherited conditions that run in families like xeroderma pigmentosum, polydysplastic epidermolysis bullosa, or Bloom syndrome may predispose one to oral SCC cancer.
9.Nutrition: Iron deficiency and vitamin A deficiency associated with Plummer-Vinson syndrome which is linked to oral and pharyngeal cancers. Nitrosamine-rich fish diet in many regions is associated with nasopharyngeal carcinoma (nose cancer).
3.DNA defect: people with xeroderma pigmentosum have a deficiency in an enzyme which is needed for normal DNA repair and are more prone to of the develop SCC.
4.Immunosupression: Patients with HIV/AIDS, cancers (like lymphoproliferative conditions) and those taking immunosuppressing drugs e.g. organ transplant patients are at risk of developing SCC.
5.Smoking: tobacco usage has been associated with increased risk of most cancers especially head and neck SCC.
6.Alcohol: Drinking excessively is associated with increased risk of SCC head and neck just like smoking.
7.Age: with increasing age, there is increased risk of cancers in general.
8.Familial associated inherited conditions: Certain inherited conditions that run in families like xeroderma pigmentosum, polydysplastic epidermolysis bullosa, or Bloom syndrome may predispose one to oral SCC cancer.
9.Nutrition: Iron deficiency and vitamin A deficiency associated with Plummer-Vinson syndrome which is linked to oral and pharyngeal cancers. Nitrosamine-rich fish diet in many regions is associated with nasopharyngeal carcinoma (nose cancer).
10.Occupational exposure to industrial metals and products: Arsenic exposure is a known risk for head and neck cancers.
11.Long standing leg ulcers: certain long standing non-healing ulcers maybe SCC. Biopsy is warranted if the lesion is suspicious.
12.Viruses: EBV virus have been associated with nasopharyngeal carcinoma (nose cancer). HIV is associated with Kaposi sarcoma. HPV is associated with genital and cervical cancer.
11.Long standing leg ulcers: certain long standing non-healing ulcers maybe SCC. Biopsy is warranted if the lesion is suspicious.
12.Viruses: EBV virus have been associated with nasopharyngeal carcinoma (nose cancer). HIV is associated with Kaposi sarcoma. HPV is associated with genital and cervical cancer.
13.Radiation exposure: ionizing radiation exposure during work or for medical treatment predispose one to cancer.
Clinical presentation of SCC
SCC may develop from pre-existing pre-cancerous lesions like actinic keratosis (scaly skin-colored to brown plaques or papules with a red base), keratoacanthoma & Bowen Dermatoses or from non-healing longstanding ulcers on sun-exposed skin surface areas. About 70% of all skin SCCs occur on the head and neck, especially over the lower lip, external ear, and the forehead and scalp, with an another 15% found on the upper extremities.
Clinical presentation of SCC
SCC may develop from pre-existing pre-cancerous lesions like actinic keratosis (scaly skin-colored to brown plaques or papules with a red base), keratoacanthoma & Bowen Dermatoses or from non-healing longstanding ulcers on sun-exposed skin surface areas. About 70% of all skin SCCs occur on the head and neck, especially over the lower lip, external ear, and the forehead and scalp, with an another 15% found on the upper extremities.
The classic presentation of SCC is a shallow ulcer with heaped-up edges, often covered by a plaque. The surface of typical SCC may go through changes like scaling, crusting, ulceration, or the presence of a cutaneous horn. They may vary from few millimeters to centimeters. Often they grow slowly and progressively. The regional lymph nodes should also be examined to determine if the cancer has spread to the lymphatic system.
The size and location of the lesion should be taken into consideration as it may affect the prognosis and cosmetic result post removal. Lesions larger than 2 cm have a higher rate of recurrence and metastasis (distant spread of cancer to other organs). Lesions with a depth greater than 4 mm have a higher rate of metastatic (distant) spread. Lesions around the ear&lip region, with perineural invasion (invades the nerves) and with histology bearing poorly differentiated and undifferentiated cellular pattern are considered as high risk lesions.
Staging and prognosis of SCC
Staging is often done using the American Joint Committee on Cancer (AJCC)/International Union against Cancer (UICC) which uses the TNM (Tumor, Nodes & Metastasizes) system.
Staging is often done using the American Joint Committee on Cancer (AJCC)/International Union against Cancer (UICC) which uses the TNM (Tumor, Nodes & Metastasizes) system.
For early stages of SCC, the 5 year survival rate is as high as >90%. The recurrence rate is as low as < 10%. For more advanced stage of SCC that has spread to lymph nodes, the 5 year survival rate is lower estimated at 25-45%. For those with distant spread of cancer to other organs the 5 year survival rate drops to about 2-5%.
Diagnosis of SCC
With the clinical history and clinical features, diagnosis of SCC can be made. Laboratory tests is often not necessary. If distant spread of cancer is suspected then imaging like Chest X-ray, CT scan and MRI scan can be done. Any lesion suspicious of being SCC should undergo a biopsy for histological confirmation. A full thickness biopsy is the standard as it can determine the depth of invasion and extent of invasion of the cancer.
Diagnosis of SCC
With the clinical history and clinical features, diagnosis of SCC can be made. Laboratory tests is often not necessary. If distant spread of cancer is suspected then imaging like Chest X-ray, CT scan and MRI scan can be done. Any lesion suspicious of being SCC should undergo a biopsy for histological confirmation. A full thickness biopsy is the standard as it can determine the depth of invasion and extent of invasion of the cancer.
Patients with lymph node involved should undergo Fine Needle Aspiration (FNA) biopsy to determine if cancer cells have spread to the lymph nodes.
Treatment of SCC
Treatment options depend on the site, size and location of SCC lesion. There are surgical and non-surgical treatments which includes topical treatment, photodynamic therapy, cryotherapy, and chemotherapy and radiation therapy.
Treatment options depend on the site, size and location of SCC lesion. There are surgical and non-surgical treatments which includes topical treatment, photodynamic therapy, cryotherapy, and chemotherapy and radiation therapy.
Surgical treatment of SCC
Surgical treatment remains the standard treatment for both skin and Head and Neck SCC cancers. For skin SCC, electrodessication and curettage/curettage and electrosurgery is less effective for recurrent lesions or those that cancer cells that invade the subcutaneous tissue.
Excision of both primary and recurrent tumors with clear margins is recommended. If the cancer is large, a flap or graft may be needed to cover the defect post-surgery.
Surgical treatment remains the standard treatment for both skin and Head and Neck SCC cancers. For skin SCC, electrodessication and curettage/curettage and electrosurgery is less effective for recurrent lesions or those that cancer cells that invade the subcutaneous tissue.
Excision of both primary and recurrent tumors with clear margins is recommended. If the cancer is large, a flap or graft may be needed to cover the defect post-surgery.
Mohs micrographic surgery, for recurrent tumors and primary lesions which are ill-defined and deep is recommended. Laser surgery can also be used for excision or destruction of superficial SCC and aids in ensuring hemostasis.
Cryotherapy
Cryotherapy uses liquid nitrogen to cool small squamous cell carcinomas (SCCs) to temperatures that can kill the cancer cells. It is only suitable for those with selected in situ squamous cell carcinomas (SCCISs) and actinic keratoses and is not suitable for invasive cancers.
It is a safe and low-cost procedure and is very useful in patients with bleeding disorders, those who refuse surgery/ poor surgical candidates, or in patients whereby surgery is contraindicated. The 5 year survival rate for superficial early stage SCC in situ can be as high as 95%. The side effects include transient localized pain, swelling, pigmentation changes, loss of hair over hair-bearing areas and blistering.
Cryotherapy uses liquid nitrogen to cool small squamous cell carcinomas (SCCs) to temperatures that can kill the cancer cells. It is only suitable for those with selected in situ squamous cell carcinomas (SCCISs) and actinic keratoses and is not suitable for invasive cancers.
It is a safe and low-cost procedure and is very useful in patients with bleeding disorders, those who refuse surgery/ poor surgical candidates, or in patients whereby surgery is contraindicated. The 5 year survival rate for superficial early stage SCC in situ can be as high as 95%. The side effects include transient localized pain, swelling, pigmentation changes, loss of hair over hair-bearing areas and blistering.
Photodynamic therapy
In photodynamic therapy, a photosensitizing drug, light, and oxygen are used to induce targeted cell death of cancerous or abnormal tissue. It is suitable for SCC in situ and actinic keratosis. There may be a higher rate of recurrence with this method as compared with surgical excision.
In photodynamic therapy, a photosensitizing drug, light, and oxygen are used to induce targeted cell death of cancerous or abnormal tissue. It is suitable for SCC in situ and actinic keratosis. There may be a higher rate of recurrence with this method as compared with surgical excision.
Radiation therapy
Radiation therapy as the only mode of therapy is only reserved for patients who are unfit for surgery. Radiation therapy is usually used as an adjunct therapy for patients post-surgery who has disease which has spread to nerves/lymph nodes or cancer with poorly defined margins. Treatment is usually given 3-5 times a week for about 1-2 months.
The side effects include localized redness, erosions, alopecia (loss of hair), localized pain, skin atrophy, pigmentation changes and telangiectasia (blood vessel dilatation) in the radiation site.
Radiation therapy as the only mode of therapy is only reserved for patients who are unfit for surgery. Radiation therapy is usually used as an adjunct therapy for patients post-surgery who has disease which has spread to nerves/lymph nodes or cancer with poorly defined margins. Treatment is usually given 3-5 times a week for about 1-2 months.
The side effects include localized redness, erosions, alopecia (loss of hair), localized pain, skin atrophy, pigmentation changes and telangiectasia (blood vessel dilatation) in the radiation site.
Chemotherapy
Systemic chemotherapy will be used for advance SCC that has spread to other organs.
Systemic chemotherapy will be used for advance SCC that has spread to other organs.
Topical treatment
Topical imiquimod is an immune modulator that is approved to treatgenital warts, actinic keratosis, Bowen disease and superficial SCC. It should be applied 3 times per week for 4-6 weeks. Localized side effects include increased redness, swelling, and erosions or ulcerations. If applied over large areas, it may cause flu-like symptoms.
Topical imiquimod is an immune modulator that is approved to treatgenital warts, actinic keratosis, Bowen disease and superficial SCC. It should be applied 3 times per week for 4-6 weeks. Localized side effects include increased redness, swelling, and erosions or ulcerations. If applied over large areas, it may cause flu-like symptoms.
Topical chemotherapy agent like 5-fluorouracil have been used for the treatment of actinic keratosis, SCC in situ and superficial BCC. They should be applied daily for about a month. It can cause skin irritation and redness over the application site.
Follow up
In general, sunscreens should be used and sun exposure should be reduced. Alcohol and tobacco use should be cut. All patients with SCC post-surgery should be followed up with dermatologists to watch for recurrence of SCC. Patients with advance disease may need follow up scans. Any recurrence should be treated aggressively.
In general, sunscreens should be used and sun exposure should be reduced. Alcohol and tobacco use should be cut. All patients with SCC post-surgery should be followed up with dermatologists to watch for recurrence of SCC. Patients with advance disease may need follow up scans. Any recurrence should be treated aggressively.
