
What is Anal Cancer?
Anal cancer is the cancer of the anus. Anus is the end of the large intestine below the rectum where the stools (feces) leave the body. The anal canal from the end of rectum to the anal opening is about 1.5 inches long. There are 2 ring-link sphincter muscles which relaxes to let the stools out of body and constricts to prevent leakage.
Anal cancer is relatively uncommon and only constitutes 1-2% of gastrointestinal cancers. In USA, about 6000 new cases of anal cancer has been diagnosed yearly.
Anal cancer is the cancer of the anus. Anus is the end of the large intestine below the rectum where the stools (feces) leave the body. The anal canal from the end of rectum to the anal opening is about 1.5 inches long. There are 2 ring-link sphincter muscles which relaxes to let the stools out of body and constricts to prevent leakage.
Anal cancer is relatively uncommon and only constitutes 1-2% of gastrointestinal cancers. In USA, about 6000 new cases of anal cancer has been diagnosed yearly.
What causes Anal Cancer?
Anal cancer occur when the normal cells undergo genetic mutation and form abnormal cancerous cells. The cancer cells grow and multiply and form a cancerous mass called tumor. In late stage, the cancer cells may spread to other organs (metastasize).
Most anal cancers are squamous cell carcinoma arising from the squamous cells that line the anal margin and most of the anal canal. Adenocarcinomas form a smaller portion of anal cancer. It is derived from cells lining the upper part of the anus near the rectum or in glands located under the anal mucosa. They are treated like rectal cancer.
Anal cancer occur when the normal cells undergo genetic mutation and form abnormal cancerous cells. The cancer cells grow and multiply and form a cancerous mass called tumor. In late stage, the cancer cells may spread to other organs (metastasize).
Most anal cancers are squamous cell carcinoma arising from the squamous cells that line the anal margin and most of the anal canal. Adenocarcinomas form a smaller portion of anal cancer. It is derived from cells lining the upper part of the anus near the rectum or in glands located under the anal mucosa. They are treated like rectal cancer.
Risk factors for Anal Cancer
There are a number of risk factors which increases a person’s chance of developing anal cancer. These include:
1. HPV infection: A sexually transmitted disease that is associated with anal cancer and other cancers which will be described on other pages on this website.
2. Sexual practice: People who have multiple sexual partners, practice unprotected sex, men who have sex with men and those who practice anal sex are at higher risk of HPV infection and anal cancer.
3. Increasing age: most anal cancers occur in patients older than 50 years old.
4. Smoking: Nicotine is carcinogenic (cancer causing chemicals) hence it not only increases the risk of anal cancer but also other cancers.
5. Immune suppression: drugs that suppress immune system (e.g. steroids, azathioprine, and ciclosporin), post organ transplants and conditions like HIV which suppress the immune state will increase risk of developing anal cancer.
6. Chronic local inflammation: Long standing anal fissures, fistulas (abnormal openings) and open wounds around the anal region also increases the chance of anal cancer.
7. Radiation: pelvic radiation to treat other cancers like prostate, rectum, bladder and cervix increases free radicals and cancer cells formation.
There are a number of risk factors which increases a person’s chance of developing anal cancer. These include:
1. HPV infection: A sexually transmitted disease that is associated with anal cancer and other cancers which will be described on other pages on this website.
2. Sexual practice: People who have multiple sexual partners, practice unprotected sex, men who have sex with men and those who practice anal sex are at higher risk of HPV infection and anal cancer.
3. Increasing age: most anal cancers occur in patients older than 50 years old.
4. Smoking: Nicotine is carcinogenic (cancer causing chemicals) hence it not only increases the risk of anal cancer but also other cancers.
5. Immune suppression: drugs that suppress immune system (e.g. steroids, azathioprine, and ciclosporin), post organ transplants and conditions like HIV which suppress the immune state will increase risk of developing anal cancer.
6. Chronic local inflammation: Long standing anal fissures, fistulas (abnormal openings) and open wounds around the anal region also increases the chance of anal cancer.
7. Radiation: pelvic radiation to treat other cancers like prostate, rectum, bladder and cervix increases free radicals and cancer cells formation.
Symptoms of Anal Cancer
About 20% of patients with anal cancer may not have any symptoms. Common symptoms include bleeding from the anus/rectum, persistent pain/itch around the anal region, sensation/presence of a lump in the anal area and mucus or pus discharge from anal canal.
Other symptoms similar to colorectal cancer include passing out blood, change in bowel pattern (more or fewer bowel movements with strain), change in stool consistency (shapeless watery forms) and presence of swollen nodes in the groin/anal area which suggest localized spread of cancer to lymphatic drainage.
Constitutional symptoms like lethargy, loss of weight and loss of appetite may suggest more advance disease. Anal cancer commonly metastasize (spread) to the liver and the lungs.
About 20% of patients with anal cancer may not have any symptoms. Common symptoms include bleeding from the anus/rectum, persistent pain/itch around the anal region, sensation/presence of a lump in the anal area and mucus or pus discharge from anal canal.
Other symptoms similar to colorectal cancer include passing out blood, change in bowel pattern (more or fewer bowel movements with strain), change in stool consistency (shapeless watery forms) and presence of swollen nodes in the groin/anal area which suggest localized spread of cancer to lymphatic drainage.
Constitutional symptoms like lethargy, loss of weight and loss of appetite may suggest more advance disease. Anal cancer commonly metastasize (spread) to the liver and the lungs.
Physical signs of Anal Cancer
Physician will take a general history looking for symptoms suggesting of anal cancer and then do a physical examination with focus on the abdomen and anal area.
Physician will take a general history looking for symptoms suggesting of anal cancer and then do a physical examination with focus on the abdomen and anal area.
Abdomen examination to look for enlarged liver which may suggest spread of cancer and also to look for enlarged lymph nodes which suggest lymphatic spread of cancer. The anus area is examined for any mass. Digital rectal examination is necessary and the physician will insert a gloved up finger into the anus opening to feel for any mass in the rectum/anal region. Sometimes a proctoscope which is an instrument is inserted via the anus to visualize the anus/rectum looking for gross cancer mass.
Diagnostic test for Anal Cancer
Before the confirmation of anal cancer, a series of investigations can be done to attain diagnosis. These include:
1. Anoscopy: A short lighted tube is inserted through the anus to visualize the rectum and anal canal. If suspicious mass is seen a biopsy is done.
Before the confirmation of anal cancer, a series of investigations can be done to attain diagnosis. These include:
1. Anoscopy: A short lighted tube is inserted through the anus to visualize the rectum and anal canal. If suspicious mass is seen a biopsy is done.
2. Colonoscopy: It is a diagnostic procedure whereby a tube with a video camera is inserted through your anus upwards to visualize the whole colon. If a polyp is seen, biopsy of the polyp and removal can be done during this procedure.
3. Endo-anal or endorectal ultrasound: an imaging procedure whereby the ultrasound probe is inserted into the anus and high energy ultrasound waves are used to create an image of the body tissues.
4. Biopsy: Small samples of tissues from suspicious cancerous mass found during scopes will be taken and examined under microscopy by pathologist to determine presence of cancer cells.
5. Imaging studies: once anal cancer is confirmed, Chest X-ray, CT scans, MRI scans and PET scans will be ordered to determine the stage of anal cancer and to see if the cancer has spread to other organs.
Stages of Anal Cancer
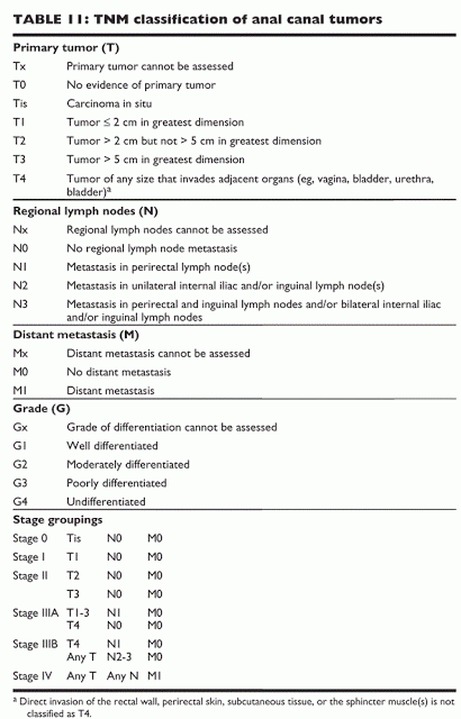
Staging of anal cancer is done by determining the size of anal cancer and whether it has spread to lymph nodes and other organs. The stages of anal cancer will affect the treatment modality and also the prognosis of the cancer.
Staging of Anal Cancer is by the TNM (Tumor Nodal Metastasis system) as described by table below.
Staging of anal cancer is done by determining the size of anal cancer and whether it has spread to lymph nodes and other organs. The stages of anal cancer will affect the treatment modality and also the prognosis of the cancer.
Staging of Anal Cancer is by the TNM (Tumor Nodal Metastasis system) as described by table below.
Treatment of Anal Cancer
The treatment plan for anal cancer depends on the stage of the disease, patient’s general health and patient’s wishes. The 3 main modalities of treatment is chemotherapy, radiation therapy and surgery.
For Stage 1-3 anal cancer which has not spread to distant organs, the standard treatment is combination of chemotherapy (5-fluorouracil and mitomycin) and radiation therapy. Small tumors can be removed surgically via local resection. For Stage 4 anal cancer that has spread to distant organs, the treatment modality is systemic chemotherapy (cisplatin and 5-fluorouracil).
The treatment plan for anal cancer depends on the stage of the disease, patient’s general health and patient’s wishes. The 3 main modalities of treatment is chemotherapy, radiation therapy and surgery.
For Stage 1-3 anal cancer which has not spread to distant organs, the standard treatment is combination of chemotherapy (5-fluorouracil and mitomycin) and radiation therapy. Small tumors can be removed surgically via local resection. For Stage 4 anal cancer that has spread to distant organs, the treatment modality is systemic chemotherapy (cisplatin and 5-fluorouracil).
Salvage therapy is reserved for patients who have persistent or recurrent anal cancer even after chemotherapy and radiotherapy. Local recurrences may be successfully salvaged with surgery.
For patients who are immune-suppressed for example HIV patients, the dose of chemotherapy should be reduced to reduce incidence of opportunistic infections.
For patients who are immune-suppressed for example HIV patients, the dose of chemotherapy should be reduced to reduce incidence of opportunistic infections.
Chemotherapy: Drugs are given to stop the growth of cancer cells, either by stopping the cells from or dividing or by killing the cells. Systemic chemotherapy involves ingesting/intravenous injection of chemotherapy drugs resulting in killing healthy and cancerous cells result in more side effects. Regional chemotherapy involves targeting chemotherapy drugs at certain organs affected. Side effects include gastrointestinal side effects (nausea, vomiting and diarrhea), hair loss, marrow suppression and opportunistic infections.
Radiotherapy: uses high-energy x-rays or other types of radiation to kill cancer cells. Internal radiation involves insertion of a device into target organ to release the x-ray radiation. External radiation involves a machine outside the body that send radiation rays to the cancer. Side effects include skin redness, sores and exposing healthy tissue to radiation damage.
Surgery: Local resection for small anal cancer involves removing the cancer with a margin of healthy tissues. This procedure seldom disrupts the sphincter muscles that control bowel movements.
Abdominoperineal resection (APR) is a surgical procedure for more advance anal cancer patients whereby the anus, rectum, part of the sigmoid colon and lymph nodes involved are removed. The end of the intestine is then brought to the skin surface called stoma forming a colostomy whereby fecal matters will empty into a bag called stoma bag. Colostomy is permanent.
Follow up
Post treatment, patients are follow up at regular intervals to look for any recurrence of disease or treatment failures. They will undergo physical examination and also further scans.
Post treatment, patients are follow up at regular intervals to look for any recurrence of disease or treatment failures. They will undergo physical examination and also further scans.
Prevention
Practice safe sex with condoms and having faithful partners will reduce chances of HIV and HPV infections associated with anal cancers.
HPV vaccination is also beneficial in preventing contacting HPV infection.
Abstain from smoking as it increases risk of anal cancer.
Practice safe sex with condoms and having faithful partners will reduce chances of HIV and HPV infections associated with anal cancers.
HPV vaccination is also beneficial in preventing contacting HPV infection.
Abstain from smoking as it increases risk of anal cancer.
