
What is Hepatic Carcinoma?
Hepatic Carcinoma/ Hepatocellular Carcinoma HCC are the cancer of the liver. Primary Liver Cancer arrives from the liver hepatocytes whereas Secondary liver cancer is spread of cancer from other organs (colon, lung, breast, pancreas and stomach) to the liver.
Hepatic carcinoma is the 8th most common cancer in women and 5th most common cancer in men worldwide. It occurs more commonly in men than women. There is about 560,000 new cases worldwide every year. Age of diagnosis is usually over 50. It is highest in areas where hepatitis B and C infections is prevalent as in Asia and sub-Saharan Africa. Hepatitis B vaccination has greatly reduced the incidence of Hepatic carcinoma.
The median survival from the time of diagnosis is about 6 months. Survival rate greatly depends on the extent of liver cirrhosis (chronic disease whereby normal liver tissue is replaced with fibrous tissue and loss of liver cell function), extent on liver failure and portal vein occlusion. Death is usually caused by cachexia, variceal bleeding, hepatic failure, tumor bleeding or bleeding into the peritoneum.
Hepatic Carcinoma/ Hepatocellular Carcinoma HCC are the cancer of the liver. Primary Liver Cancer arrives from the liver hepatocytes whereas Secondary liver cancer is spread of cancer from other organs (colon, lung, breast, pancreas and stomach) to the liver.
Hepatic carcinoma is the 8th most common cancer in women and 5th most common cancer in men worldwide. It occurs more commonly in men than women. There is about 560,000 new cases worldwide every year. Age of diagnosis is usually over 50. It is highest in areas where hepatitis B and C infections is prevalent as in Asia and sub-Saharan Africa. Hepatitis B vaccination has greatly reduced the incidence of Hepatic carcinoma.
The median survival from the time of diagnosis is about 6 months. Survival rate greatly depends on the extent of liver cirrhosis (chronic disease whereby normal liver tissue is replaced with fibrous tissue and loss of liver cell function), extent on liver failure and portal vein occlusion. Death is usually caused by cachexia, variceal bleeding, hepatic failure, tumor bleeding or bleeding into the peritoneum.
Causes of Hepatic Carcinoma
1. Chronic Hepatitis B and C infection:
2. Alcohol:
3. Aflatoxin B1
4. Drugs, chemicals and medications
5. Hemochromatosis
6. Diabetes and obesity
7. Autoimmune hepatitis
8. Cirrhosis:
1. Chronic Hepatitis B and C infection:
- Hepatitis B and C infection increases the risk of hepatic carcinoma. One can contract Hepatitis B and C via infusion of contaminated blood or shared needles, sexual intercourse and through vaginal delivery at birth.
- Specific areas of Hepatitis B virus genome enter the liver cells’ genetic material and cause disruption of normal liver cells genome leading to cancerous changes in cells.
- How Hepatitis C causes hepatic carcinoma is less understood. It is postulated that hepatitis c cause liver cirrhosis which in turn lead to hepatic carcinoma.
2. Alcohol:
- Chronic excessive alcohol consumption will lead to irreversible liver damage and cirrhosis and eventually hepatic carcinoma.
3. Aflatoxin B1
- Consuming of foods that are contaminated with fungi that produce aflatoxins B1 that are very toxic to the liver. These molds/fungi can be found in contaminated food like peanuts, rice, soybeans, corn, and wheat. These aflatoxins cause mutations in the p53 gene that result in cancerous changes in liver cells.
4. Drugs, chemicals and medications
- Anabolic steroids and female hormones (estrogen) have been associated with the development of hepatic adenomas. Hepatic adenomas are benign non-cancerous growth that can evolve into cancer.
- Chronic exposure to vinyl chloride a chemical in plastics can cause hepatic angiosarcoma, a cancer of blood vessels in the liver.
5. Hemochromatosis
- An inherited disorder whereby there is excessive iron stores in the body especially the liver leading to liver cirrhosis and increased risk of hepatic carcinoma.
6. Diabetes and obesity
- Both conditions result in accumulation of fat in liver and chronic liver damage.
- The accumulation of fat in liver results in NASH (Non-alcoholic steatohepatitis) which will lead to liver cirrhosis and increased risk of hepatic carcinoma.
7. Autoimmune hepatitis
- Autoimmune diseases caused chronic damage to the liver leading to cirrhosis and eventual increased risk of hepatic carcinoma.
8. Cirrhosis:
- Liver Cirrhosis increases risk of hepatic carcinoma.
- The risk is 3-4 times higher in patients with cirrhosis than patients with hepatic infection in the general population.
Clinical Presentation of Hepatic Carcinoma
Patients will usually present with symptoms of advancing liver cirrhosis. These include:
1. Itch: as the liver function deteriorates the blood bilirubin rises resulting in extreme body itch.
2. Jaundice: As the bilirubin rises, the skin and sclera of the eyes turn yellow resulting in jaundice.
3. Hepatosplenomegaly (Enlarged liver and spleen): As the liver cancer spreads and enlarges it results in enlargement of the liver. It can also invade and block the portal vein that brings blood to the liver from the intestine and the spleen. This eventually will lead to the enlargement of the spleen.
4. Variceal bleeding: When the portal vein is blocked, this result in increased pressure in the esophageal veins resulting in dilatation of the veins forming esophageal varices that has a tendency to bleed.
5. Loss of weight and appetite: As the cancer progresses there will be a significant weight loss, loss of appetite and general lethargy.
6. Ascites: The patient will experience abdomen distension and accumulation of fluid in the peritoneum
7. Right Upper abdomen pain: As the tumor enlarges, bleeds or ruptures it will cause pain over the right upper quadrant abdomen.
8. Hepatic Encephalopathy: Late stages of liver cancer will cause liver failure and lead to confusion, altered mental status and coma.
Physical examination of the patient will reveal a jaundiced cachectic (physical wasting with loss of weight and muscle mass due to disease) patient who has abdomen ascites, enlarged liver, enlarged spleen, pedal edema (swelling of lower limbs), peri-umbilical collateral veins (dilated veins seen on the abdomen) and enlarged hemorrhoids (Piles).
Alcoholic cause of longstanding liver disease will result in dupuytren contracture (painless thickening and contracture of tissue beneath the skin on the palm of the hand and fingers) and spider naevi (A superficial spider-like cluster of capillaries beneath the skin) in the patients. In patients with hepatic encephalopathy they will have asterixis (flapping tremor of the hand), appear confused or comatose.
Patients will usually present with symptoms of advancing liver cirrhosis. These include:
1. Itch: as the liver function deteriorates the blood bilirubin rises resulting in extreme body itch.
2. Jaundice: As the bilirubin rises, the skin and sclera of the eyes turn yellow resulting in jaundice.
3. Hepatosplenomegaly (Enlarged liver and spleen): As the liver cancer spreads and enlarges it results in enlargement of the liver. It can also invade and block the portal vein that brings blood to the liver from the intestine and the spleen. This eventually will lead to the enlargement of the spleen.
4. Variceal bleeding: When the portal vein is blocked, this result in increased pressure in the esophageal veins resulting in dilatation of the veins forming esophageal varices that has a tendency to bleed.
5. Loss of weight and appetite: As the cancer progresses there will be a significant weight loss, loss of appetite and general lethargy.
6. Ascites: The patient will experience abdomen distension and accumulation of fluid in the peritoneum
7. Right Upper abdomen pain: As the tumor enlarges, bleeds or ruptures it will cause pain over the right upper quadrant abdomen.
8. Hepatic Encephalopathy: Late stages of liver cancer will cause liver failure and lead to confusion, altered mental status and coma.
Physical examination of the patient will reveal a jaundiced cachectic (physical wasting with loss of weight and muscle mass due to disease) patient who has abdomen ascites, enlarged liver, enlarged spleen, pedal edema (swelling of lower limbs), peri-umbilical collateral veins (dilated veins seen on the abdomen) and enlarged hemorrhoids (Piles).
Alcoholic cause of longstanding liver disease will result in dupuytren contracture (painless thickening and contracture of tissue beneath the skin on the palm of the hand and fingers) and spider naevi (A superficial spider-like cluster of capillaries beneath the skin) in the patients. In patients with hepatic encephalopathy they will have asterixis (flapping tremor of the hand), appear confused or comatose.
Diagnostic Tests for Hepatic Carcinoma
1. Laboratory tests
2. Liver Imaging Studies
1. Laboratory tests
- Liver Function Test: There will be elevated total bilirubin, aspartate aminotransferase (AST), alkaline phosphatase and prothrombin time consistent with liver cirrhosis. Albumin will be lowered.
- Alpha-fetoprotein (AFP): AFP is a tumor marker that will be elevated in 75% of the cases. Normal levels of AFP are below 10 ng/ml, an elevation of more than 400 ng/mL predicts for hepatic carcinoma with specificity >95%.It maybe falsely elevated in patients with hepatitis hence not effective as screening tool.
2. Liver Imaging Studies
- Ultrasonography: It is an inexpensive procedure but operator dependent. It is unable to detect small nodules. Any suspicious lesion found must be followed up with additional imaging to confirm diagnosis and for staging.
- Triphasic Ct Scan: The 3 phases are no-contrast phase, arterial phase and portal venous phase. It can be used to identify liver tumors and disease staging. However in nodular cirrhotic livers, the sensitivity for detecting hepatocellular carcinoma is low.
- MRI Scan: It can detect smaller nodules and portal vein flow. It has better sensitivity and specificity in detecting hepatic carcinoma in nodular cirrhotic livers. However it is more expensive.
- Angiography: This is an invasive procedure whereby a catheter is inserted into the femoral artery in the groin, up the aorta to hepatic artery that supplies the liver. Imaging with contrast is done to look for neovascularization (abnormal vessels that feed the liver tumor). It can also be used in chemoembolization a treatment for hepatic carcinoma.
- PET scan: currently not recommended for diagnosis and staging of hepatic carcinoma.
- Chest X-ray: to look for cancer spread to the lungs.
1. Liver Biopsy
2. Histology
- Under ultrasound/CT guidance, a needle is inserted into the liver tissue and a tissue sample is extracted.
- Core biopsy is preferred over fine needle biopsy to make the diagnosis.
- Some studies suggest small chance of tumor seeding during procedure whereas some studies show no difference. Other risks involved bleeding and infection.
- If imaging shows an enlarging liver mass and a high level of AFP (500-1000 ng/ml) it is diagnostic of hepatic carcinoma and biopsy may be omitted.
- Biopsy samples are sent for histology confirmation of hepatocellular carcinoma.
2. Histology
- The biopsy sample is then examined under microscopic to examine the cell type and how differentiated the cells are to confirm diagnosis of hepatic carcinoma.
- The histology can ranged from well-differentiated tumors to anaplastic tumors.
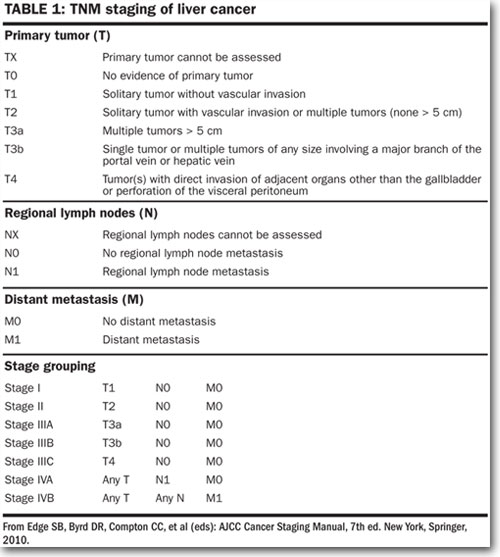
Staging of Hepatocellular Carcinoma
Staging of hepatic carcinoma is by the TNM system which involves the Tumor invasion extent, lymph Nodes involved and whether there is metastasis (spread of cancer to other organs).
Staging of hepatic carcinoma is by the TNM system which involves the Tumor invasion extent, lymph Nodes involved and whether there is metastasis (spread of cancer to other organs).
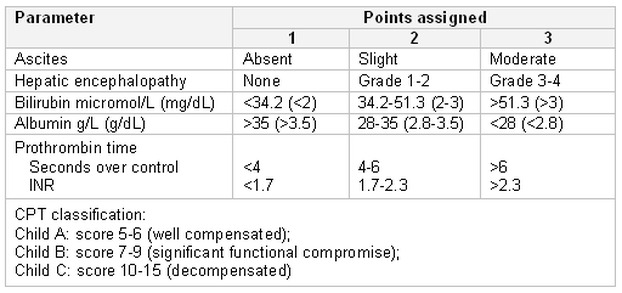
Hepatic carcinoma is strongly associated with liver cirrhosis. Liver cirrhosis is the result of longstanding liver disease causing normal liver cells to be replaced by fibrous and scar tissue eventually resulting in liver failure.
Liver cirrhosis severity is classified by Child-Pugh scoring which determine the severity of liver disease on the basis of serum albumin, bilirubin, prothrombin time, ascites , and encephalopathy .The higher the score the more severe the liver disease.
Liver cirrhosis severity is classified by Child-Pugh scoring which determine the severity of liver disease on the basis of serum albumin, bilirubin, prothrombin time, ascites , and encephalopathy .The higher the score the more severe the liver disease.
CLIP Scoring
There is a system called CLIP (Cancer of the Liver Italian Program) scoring system that predicts the median survival time and overall prognosis of patients with liver cancer. The score ranges from 0-6 and is based on Child-Pugh stage, tumor morphology, alpha-fetoprotein level and portal vein thrombosis.
Score of 0-2 is assigned to the 4 features and cumulative score system is calculated using the CLIP system as illustrated below:
1. Child-Pugh Score
2. Tumor morphology
3. Alpha-fetoprotein level
Estimated survival based on the CLIP Score:
There is a system called CLIP (Cancer of the Liver Italian Program) scoring system that predicts the median survival time and overall prognosis of patients with liver cancer. The score ranges from 0-6 and is based on Child-Pugh stage, tumor morphology, alpha-fetoprotein level and portal vein thrombosis.
Score of 0-2 is assigned to the 4 features and cumulative score system is calculated using the CLIP system as illustrated below:
1. Child-Pugh Score
- Child Pugh A: 0 point
- Child Pugh B: 1 point
- Child Pugh C: 2 points
2. Tumor morphology
- Single nodule with extension < 50%: 0 point
- Multiple nodules with extension < 50%: 1 point
- Massive tumor with extension >50%: 2 points
3. Alpha-fetoprotein level
- < 400 : 0 point
- > 400: 1 point
- Absent: 0 point
- Present: 1 point
Estimated survival based on the CLIP Score:
- Patients with a total CLIP score of 0 have an estimated survival of 31 months
- Patients with score of 1 has estimated survival of 27 months
- Patients with score of 2 has estimated survival of 13 months
- Patients with score of 3 has estimated survival of 8 months
- Patients with scores 4-6 have estimated survival of 2 months.
Treatment of Hepatic Carcinoma
The treatment modalities available for liver cancer depend on a variety of factors like the size, location and number of tumors, whether there is liver cirrhosis, has the cancer spread to other organs, the functional status of the patient, suitability for liver transplant, patency of the portal vein and other co-morbid diseases.
The overall survival rate of a patient with liver cancer symptoms is about 2-3 months. Before commencing treatment, complications of liver cancer like cirrhosis, ascites, variceal bleeding, hepatic encephalopathy and spontaneous bacteria peritonitis should be treated first. Treatment is aim to prolong life without compromising quality of life.
Liver transplant and surgery resection are the only chances of cure. Suitability depends on the tumor size, the remaining liver function and if the cancer has spread. So far only about 5% of patients are suitable for liver transplant which has about 75% of 5 year survival rate and a cancer recurrence of less than 15% in 5 years.
Other localized treatments include chemoembolization, ethanol ablation, radiofrequency ablation, cryoablation, and radiotherapy. In very advanced cases, systemic chemotherapy may be used.
The treatment modalities available for liver cancer depend on a variety of factors like the size, location and number of tumors, whether there is liver cirrhosis, has the cancer spread to other organs, the functional status of the patient, suitability for liver transplant, patency of the portal vein and other co-morbid diseases.
The overall survival rate of a patient with liver cancer symptoms is about 2-3 months. Before commencing treatment, complications of liver cancer like cirrhosis, ascites, variceal bleeding, hepatic encephalopathy and spontaneous bacteria peritonitis should be treated first. Treatment is aim to prolong life without compromising quality of life.
Liver transplant and surgery resection are the only chances of cure. Suitability depends on the tumor size, the remaining liver function and if the cancer has spread. So far only about 5% of patients are suitable for liver transplant which has about 75% of 5 year survival rate and a cancer recurrence of less than 15% in 5 years.
Other localized treatments include chemoembolization, ethanol ablation, radiofrequency ablation, cryoablation, and radiotherapy. In very advanced cases, systemic chemotherapy may be used.
Surgery treatment
Surgery provides the best possibility of a cure. In United States, only 5% of patients are suitable for surgical resection. Patients who have solitary hepatocellular carcinoma with no invasions of vessels and a well preserved liver function have the best outcomes from surgery. Many surgeons use a tumor size of < 5 cm as a cut off on tumor size criteria.
The 5 year survival rates for those who undergone liver resection ranges from 30% to 90%. The liver has the capability to regenerate post resection. A healthy liver can have up to 75% removed and the remainder tissue will regenerate to normal size in 6 months. However, in patients with liver cirrhosis the regeneration may be limited.
The liver has right and left lobes divided into a total of 8 segments. The liver surgical resections include resection of either the right/left lobe, extended lobectomy (more than 1 lobe resection) or segmental lobectomy (part of a lobe).
Surgery provides the best possibility of a cure. In United States, only 5% of patients are suitable for surgical resection. Patients who have solitary hepatocellular carcinoma with no invasions of vessels and a well preserved liver function have the best outcomes from surgery. Many surgeons use a tumor size of < 5 cm as a cut off on tumor size criteria.
The 5 year survival rates for those who undergone liver resection ranges from 30% to 90%. The liver has the capability to regenerate post resection. A healthy liver can have up to 75% removed and the remainder tissue will regenerate to normal size in 6 months. However, in patients with liver cirrhosis the regeneration may be limited.
The liver has right and left lobes divided into a total of 8 segments. The liver surgical resections include resection of either the right/left lobe, extended lobectomy (more than 1 lobe resection) or segmental lobectomy (part of a lobe).
Liver Transplantation
Liver transplantation not only eliminates the cancer and also cures underlying liver disease. It can be considered in patients who meet Milan Criteria: tumor less than 5 cm or up to 3 tumors which are less than 3 cm. 5 year survival rate is about 50-60%.
Liver transplantation not only eliminates the cancer and also cures underlying liver disease. It can be considered in patients who meet Milan Criteria: tumor less than 5 cm or up to 3 tumors which are less than 3 cm. 5 year survival rate is about 50-60%.
Localized Treatment modalities
Those who do not fulfill the criteria for surgical treatment can undergo localized treatments.
Radiofrequency Ablation (RFA)
Under ultrasound guidance, a RFA needle probe is inserted into the tumor, a high frequency alternating current is developed to the electrode, heating up the tumor tissue above 60 degrees resulting in the tumor cells to die and necrosis.
This procedure is suitable for tumors less than 4 cm in size. The local recurrence rate is about 5-6 % in 20 months. Larger tumors have a higher recurrence rates. However patients eventually develop liver/extra-liver diseases from pre-existing micro-satellite cancer lesions.
RFA is usually very well tolerated. Possible complications include bleeding, pain, fever, hematoma (bruise), intermittent transaminitis (deranged liver function tests) and pleural effusion (collection of fluid in the pleura of lungs).
Those who do not fulfill the criteria for surgical treatment can undergo localized treatments.
Radiofrequency Ablation (RFA)
Under ultrasound guidance, a RFA needle probe is inserted into the tumor, a high frequency alternating current is developed to the electrode, heating up the tumor tissue above 60 degrees resulting in the tumor cells to die and necrosis.
This procedure is suitable for tumors less than 4 cm in size. The local recurrence rate is about 5-6 % in 20 months. Larger tumors have a higher recurrence rates. However patients eventually develop liver/extra-liver diseases from pre-existing micro-satellite cancer lesions.
RFA is usually very well tolerated. Possible complications include bleeding, pain, fever, hematoma (bruise), intermittent transaminitis (deranged liver function tests) and pleural effusion (collection of fluid in the pleura of lungs).
Cryoablation
Under ultrasound guidance, the liquid nitrogen filled probe is targeted on tumors less than 5cm and using sub-zero temperatures it is used to freeze the cancer cells destroying them. This procedure is well tolerated.
Under ultrasound guidance, the liquid nitrogen filled probe is targeted on tumors less than 5cm and using sub-zero temperatures it is used to freeze the cancer cells destroying them. This procedure is well tolerated.
Percutaneous ethanol or acetic acid ablation
Under ultrasound guidance, percutaneous injection of ethanol/acetic acid into the tumor causing the cancer cells to die. This procedure is reserved for patients with small tumors. Currently Radiofrequency Ablation treatment is more favorable than this older technique.
Under ultrasound guidance, percutaneous injection of ethanol/acetic acid into the tumor causing the cancer cells to die. This procedure is reserved for patients with small tumors. Currently Radiofrequency Ablation treatment is more favorable than this older technique.
CyberKnife
This is a new technology combining robotics and imaging guidance to deliver concentrated and highly focused radiation beams to the targeted hepatic carcinoma while avoiding radiation to other healthy tissues. Currently only few medical centers have this technology and long term effects is still unknown.
This is a new technology combining robotics and imaging guidance to deliver concentrated and highly focused radiation beams to the targeted hepatic carcinoma while avoiding radiation to other healthy tissues. Currently only few medical centers have this technology and long term effects is still unknown.
Chemoembolization
Chemoembolization is a chemotherapy treatment whereby high concentrations of chemotherapy drugs are injected into the hepatic artery which usually supplies the cancer tissue. The normal liver tissues usually get blood supply from the portal vein system. Up to 85% of the anti-cancer drugs are trapped in the liver hence minimizing the systemic side effects.
Chemoembolization is a chemotherapy treatment whereby high concentrations of chemotherapy drugs are injected into the hepatic artery which usually supplies the cancer tissue. The normal liver tissues usually get blood supply from the portal vein system. Up to 85% of the anti-cancer drugs are trapped in the liver hence minimizing the systemic side effects.
Radioembolization
Selected internal radiotherapy involves targeting the liver cancer cells with yttrium-90 radiation to cause cancer cells necrosis. It is suitable for patients with portal vein thrombosis which may not be able to go through chemoembolization.
Selected internal radiotherapy involves targeting the liver cancer cells with yttrium-90 radiation to cause cancer cells necrosis. It is suitable for patients with portal vein thrombosis which may not be able to go through chemoembolization.
Chemotherapy
For patients who are not suitable for liver surgery, liver transplant or localized tumor ablation modalities, systemic chemotherapy is the mainstay treatment. However hepatic carcinoma responds poorly to chemotherapy.
Chemotherapy systemic side effects are usually less well-tolerated as compared to localized tumor ablation options. By far, the most effective chemotherapy drugs include Cisplatin, Fluorouracil and Doxorubicin. Response rate is about 10%.
Using immune-modulatory drugs like interferon-alpha in conjunction with chemotherapy may increase response rates to 20% but the treatment related toxicity is significant.
For patients who are not suitable for liver surgery, liver transplant or localized tumor ablation modalities, systemic chemotherapy is the mainstay treatment. However hepatic carcinoma responds poorly to chemotherapy.
Chemotherapy systemic side effects are usually less well-tolerated as compared to localized tumor ablation options. By far, the most effective chemotherapy drugs include Cisplatin, Fluorouracil and Doxorubicin. Response rate is about 10%.
Using immune-modulatory drugs like interferon-alpha in conjunction with chemotherapy may increase response rates to 20% but the treatment related toxicity is significant.
Other Drugs
Anti-angiogenesis agents like bevacizumab works by disrupting the formation of new blood vessels that feed the tumor cells. When used alone, it has limited clinical use. A combination of bevacizumab with gemcitabine and oxaliplatin will produce a possible 20% response rate.
Sorafenib, a multi-targeted oral kinase inhibitor, is a new drug which has been shown to improve survival rate in the trial phase.
Anti-angiogenesis agents like bevacizumab works by disrupting the formation of new blood vessels that feed the tumor cells. When used alone, it has limited clinical use. A combination of bevacizumab with gemcitabine and oxaliplatin will produce a possible 20% response rate.
Sorafenib, a multi-targeted oral kinase inhibitor, is a new drug which has been shown to improve survival rate in the trial phase.
Follow up
Post treatment, patient should undergo regular follow up with their doctors. Imaging studies to monitor regression/progression will be done every 2-3 months. Blood tests like liver function test, Alpha-fetoprotein cancer marker should be monitored monthly.
Prevention of Liver Cancer
1. Hepatitis B vaccination: As hepatitis B infection increases the risk of hepatic carcinoma, childhood vaccination against hepatitis B has greatly reduced its incidence.
2. Reduces risk of Hepatitis B/C: As hepatitis B/C is transmitted via sexual transmission and blood transmission. One should not engage in unprotected sex, avoid intravenous drug abuse/sharing of needles and go to proper sterilized shops for piercing and tattoos. Babies born to mothers who are hepatitis B positive should get vaccinated and given hepatitis immunoglobulin at birth to reduce the risk of contraction.
3. Alcohol restriction: Excessive longstanding consumption of alcohol increases the risk of hepatic carcinoma hence cutting down the consumption of alcohol will reduce the risk of cirrhosis and eventual liver cancer.
4. Screening for inherited diseases: Hemochromatosis is a hereditary disease, screening for it in families who have positive history of the disease is important. If positive follow up with a specialist is important.
5. Avoiding Aflatoxins that are toxic to the liver. Food storage is important to avoid Aflatoxin contamination of food.
6. For those who are hepatitis B/C carrier, routine yearly ultrasound liver, 6 monthly Liver function blood tests and alpha-fetoprotein levels to detect liver cancer early to allow treatment result in better prognosis.
Post treatment, patient should undergo regular follow up with their doctors. Imaging studies to monitor regression/progression will be done every 2-3 months. Blood tests like liver function test, Alpha-fetoprotein cancer marker should be monitored monthly.
Prevention of Liver Cancer
1. Hepatitis B vaccination: As hepatitis B infection increases the risk of hepatic carcinoma, childhood vaccination against hepatitis B has greatly reduced its incidence.
2. Reduces risk of Hepatitis B/C: As hepatitis B/C is transmitted via sexual transmission and blood transmission. One should not engage in unprotected sex, avoid intravenous drug abuse/sharing of needles and go to proper sterilized shops for piercing and tattoos. Babies born to mothers who are hepatitis B positive should get vaccinated and given hepatitis immunoglobulin at birth to reduce the risk of contraction.
3. Alcohol restriction: Excessive longstanding consumption of alcohol increases the risk of hepatic carcinoma hence cutting down the consumption of alcohol will reduce the risk of cirrhosis and eventual liver cancer.
4. Screening for inherited diseases: Hemochromatosis is a hereditary disease, screening for it in families who have positive history of the disease is important. If positive follow up with a specialist is important.
5. Avoiding Aflatoxins that are toxic to the liver. Food storage is important to avoid Aflatoxin contamination of food.
6. For those who are hepatitis B/C carrier, routine yearly ultrasound liver, 6 monthly Liver function blood tests and alpha-fetoprotein levels to detect liver cancer early to allow treatment result in better prognosis.
