
What is Cervical Cancer?
Cervical cancer is the 3rd most common women cancer worldwide. It is the cancer of the cervix which is neck of the womb (uterus) that connects it to the birth canal (vagina). The incidence of late-stage cervical cancer was highest among women aged 50-79 years. The incidence is higher in developing countries compared with developed countries.
Cervical cancer is the 3rd most common women cancer worldwide. It is the cancer of the cervix which is neck of the womb (uterus) that connects it to the birth canal (vagina). The incidence of late-stage cervical cancer was highest among women aged 50-79 years. The incidence is higher in developing countries compared with developed countries.
What causes cervical cancer?
Cervical cancer commonly arise from the cells the line the cervix which undergo genetic mutation to form cancer cells which then multiple and form a cancer mass. The cancer cells can also spread locally to adjacent structures, to the lymph nodes and via blood to other distant organs (metastasize).
The pre-cancerous stage before the cells turn cancerous is called Cervical Intra-epithelial Neoplasia commonly in short called CIN.
Cervical cancer commonly arise from the cells the line the cervix which undergo genetic mutation to form cancer cells which then multiple and form a cancer mass. The cancer cells can also spread locally to adjacent structures, to the lymph nodes and via blood to other distant organs (metastasize).
The pre-cancerous stage before the cells turn cancerous is called Cervical Intra-epithelial Neoplasia commonly in short called CIN.
Human Papillomavirus (HPV) infection is a sexually transmitted diseasewhich play a huge role in cervical cancer development. 5% of HPV infections will result in CIN grade 2 or 3 lesions within 3 years of infection. 20% of CIN 3 lesions progress to invasive cervical cancer within 5 years. About 40% of CIN 3 lesions progress to invasive cervical cancer within 30 years.
The factors that contribute to development of CIN 3 include persistent infection of high risk HPV type, immune-compromised stats e.g. HIV, smoking, vitamin deficiency states and lack of screening test like Pap smears for early detection. Certain genetic susceptibility has also been related to the development of cervical cancer.
More than 90% of all cervical cancers worldwide are caused by 8 HPV types: 16, 18, 31, 33, 35, 45, 52, and 58. In particular, three types (16, 18 and 45) cause 94% of cervical adenocarcinomas. HPV subtype 16 is poses the greatest risk.
The factors that contribute to development of CIN 3 include persistent infection of high risk HPV type, immune-compromised stats e.g. HIV, smoking, vitamin deficiency states and lack of screening test like Pap smears for early detection. Certain genetic susceptibility has also been related to the development of cervical cancer.
More than 90% of all cervical cancers worldwide are caused by 8 HPV types: 16, 18, 31, 33, 35, 45, 52, and 58. In particular, three types (16, 18 and 45) cause 94% of cervical adenocarcinomas. HPV subtype 16 is poses the greatest risk.
What are the risk factors for cervical cancer?
As HPV infection is related to cervical cancer, it is sometimes referred to a sex-related cancer with risk factors associated with sexual risk factors like:
1. Multiple Sexual Partners: increase your risk of contracting HPV
2. First sex at young age: increases chance of HPV as sexual partners will also increase
3. History of sexually transmitted disease
4. HIV infection and other immune compromised states: more susceptible to contracting infection and weaken immune system to fight it
5. Smoking: cigarette contains nicotine which is a cancer causing agent
6. Persistent high risk HPV infection
7. History of promiscuous male partners: Promiscuous male partners is more likely to carry not only HPV but other STD.
As HPV infection is related to cervical cancer, it is sometimes referred to a sex-related cancer with risk factors associated with sexual risk factors like:
1. Multiple Sexual Partners: increase your risk of contracting HPV
2. First sex at young age: increases chance of HPV as sexual partners will also increase
3. History of sexually transmitted disease
4. HIV infection and other immune compromised states: more susceptible to contracting infection and weaken immune system to fight it
5. Smoking: cigarette contains nicotine which is a cancer causing agent
6. Persistent high risk HPV infection
7. History of promiscuous male partners: Promiscuous male partners is more likely to carry not only HPV but other STD.
Types of Cervical Cancer
The type of cervical cancer depend on the type of cells that turn cancerous. Squamous cell carcinoma accounts for most cervical cancers. It is derived from cells that line the outer portion of the cervix, which projects into the vagina.
Adenocarcinomas arrive from glandular cells that line the cervical canal and account for smaller portions of cervical cancers. In very small number of patients both types of cancer may occur concurrently.
The type of cervical cancer depend on the type of cells that turn cancerous. Squamous cell carcinoma accounts for most cervical cancers. It is derived from cells that line the outer portion of the cervix, which projects into the vagina.
Adenocarcinomas arrive from glandular cells that line the cervical canal and account for smaller portions of cervical cancers. In very small number of patients both types of cancer may occur concurrently.
Staging of Cervical Cancer
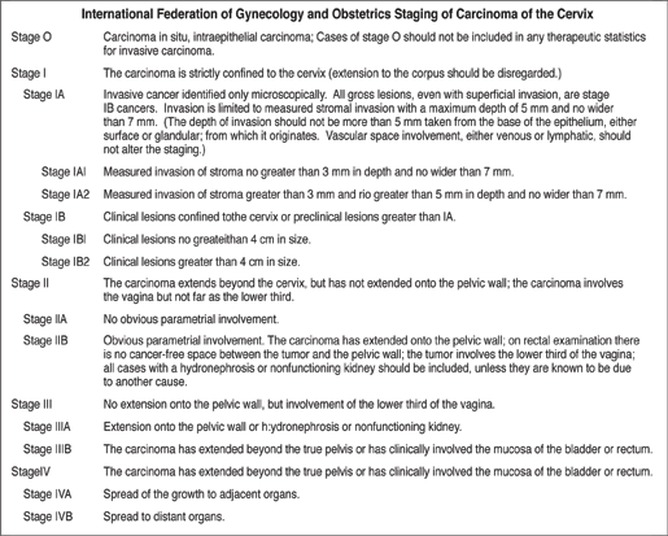
The staging of cervical cancer is commonly done using the FIGO (International Federation of Gynecology and Obstetrics). Staging of the cervical cancer aids in determining treatment plan and to estimate the prognosis of disease. The stages are:
The staging of cervical cancer is commonly done using the FIGO (International Federation of Gynecology and Obstetrics). Staging of the cervical cancer aids in determining treatment plan and to estimate the prognosis of disease. The stages are:
Prognosis of Cervical Cancer
The 5 year survival rate of cervical cancer depends on its stage:
Stage I - > 90%
Stage II - 60-80%
Stage III –50%
Stage IV - < 30%
The 5 year survival rate of cervical cancer depends on its stage:
Stage I - > 90%
Stage II - 60-80%
Stage III –50%
Stage IV - < 30%
Clinical symptoms of Cervical Cancer
Very early cancer stages do not cause any clinical symptoms. As the cancer grows it can cause the following symptoms:
1. Vaginal bleeding especially after sex
2. Abnormal bleeding in between periods or after menopause
3. Pain/discomfort during sexual intercourse
4. Foul smelling heavy vaginal discharge
5. If the cancer has invade the bladder it can cause hematuria (bloody urine), urine obstruction leading to hydronephrosis (swollen kidneys due to urine obstruction) and dysuria (pain on urination).
If cancer has invade the rectum, it can cause constipation and blood in stools.
6. Common sites where the cancer will spread distantly are the extra-pelvic lymph nodes, lungs, liver and bones.
Very early cancer stages do not cause any clinical symptoms. As the cancer grows it can cause the following symptoms:
1. Vaginal bleeding especially after sex
2. Abnormal bleeding in between periods or after menopause
3. Pain/discomfort during sexual intercourse
4. Foul smelling heavy vaginal discharge
5. If the cancer has invade the bladder it can cause hematuria (bloody urine), urine obstruction leading to hydronephrosis (swollen kidneys due to urine obstruction) and dysuria (pain on urination).
If cancer has invade the rectum, it can cause constipation and blood in stools.
6. Common sites where the cancer will spread distantly are the extra-pelvic lymph nodes, lungs, liver and bones.
Physical signs of Cervical Cancer
Your medical physician will take a medical history from you and do a thorough physical examination not just pertaining to the pelvis but the general body as sometimes cancer may have spread to other organs.
In the initial early stages of cancer, there may be no sign at all during physical examination. As the cancer enlarges, examination of cervix using a vaginal speculum may reveal a mass, ulcer or erosions at the cervix. The physician will also do a bimanual palpation to examine for pelvic or parametrial spread of cancer.
Your medical physician will take a medical history from you and do a thorough physical examination not just pertaining to the pelvis but the general body as sometimes cancer may have spread to other organs.
In the initial early stages of cancer, there may be no sign at all during physical examination. As the cancer enlarges, examination of cervix using a vaginal speculum may reveal a mass, ulcer or erosions at the cervix. The physician will also do a bimanual palpation to examine for pelvic or parametrial spread of cancer.
Rectal examination will also be done to rule out spread of cancer to the rectum which is near to the cervix. Abdomen examination sometimes reveal an enlarged liver suggesting distant spread of cancer to the liver.
Pedal edema (swelling of the legs) may suggest an obstruction of lymphatics or blood due to the cancer mass. If the lungs are involved and there is pleural effusion, they may be clinical signs too.
Pedal edema (swelling of the legs) may suggest an obstruction of lymphatics or blood due to the cancer mass. If the lungs are involved and there is pleural effusion, they may be clinical signs too.
Diagnostic tests for Cervical Cancer
1. Pap smear: A screening test often done every 3 yearly for all sexually active patients to detect pre-cancerous cervical cancer. A speculum is inserted into the vaginal to visualize the cervix and using a brush cells are scraped from the cervix and sent to the laboratory. If any abnormalities detected, they should proceed to do a colposcopy.
1. Pap smear: A screening test often done every 3 yearly for all sexually active patients to detect pre-cancerous cervical cancer. A speculum is inserted into the vaginal to visualize the cervix and using a brush cells are scraped from the cervix and sent to the laboratory. If any abnormalities detected, they should proceed to do a colposcopy.
2. HPV DNA Test: For those above 30 years old, HPV DNA test is to determine presence of HPV virus, cervical cells are sent to the laboratory for testing using The Hybrid Capture II assay.
3. Colposcopy: An outpatient procedure using a colposcope (microscope) to look for any suspicious abnormal changes of the cervix. A biopsy will be done to send the abnormal tissue to the laboratory to test for presence of cancerous cells.
3. Colposcopy: An outpatient procedure using a colposcope (microscope) to look for any suspicious abnormal changes of the cervix. A biopsy will be done to send the abnormal tissue to the laboratory to test for presence of cancerous cells.
4. Imaging studies: If cervical cancer is confirmed, then imaging studies will be done to stage the cancer and see how far it has spread in the body. Chest x-ray, CT scan, MRI scans and PET scans are modalities to look for cancer extension.
5. Cystoscopy/proctoscopy: Cystoscopy to visualize the bladder and proctoscopy to visualize the rectum may be necessary for bulky cervix cancer to look for local spread of disease to these organs.
5. Cystoscopy/proctoscopy: Cystoscopy to visualize the bladder and proctoscopy to visualize the rectum may be necessary for bulky cervix cancer to look for local spread of disease to these organs.
Cervical cancer screening
US Preventive Services Task Force (USPSTF) and American College of Obstetricians and Gynecologists (ACOG) come up with screening recommendations for cervical cancer depending on patient’s age group:
- <25 years old: No screening required
- 21-29 years (sexually active): Pap smear every 3 years
- 30-65 years: HPV DNA test and pap smear every 5 years OR pap smear alone every 3 years
- >65 years: no need screening if previous pap smears all negative and not high risk for cervical cancer.
If Pap smear reveals abnormality, patient will proceed with HPV DNA typing and colposcopy test.
Patients who have hysterectomy (surgical removal of the womb/uterus and cervix) before can stop cervical cancer screening unless their cervix is not removed, they have a history of CIN2/3 and history of cervical cancer.
Women with atypical squamous cells of undetermined significance (ASCUS) found on Pap smear but a negative HPV test can be rescreened with (Pap smear and HPV test) in 5 years or with Pap smear alone in 3 years.
US Preventive Services Task Force (USPSTF) and American College of Obstetricians and Gynecologists (ACOG) come up with screening recommendations for cervical cancer depending on patient’s age group:
- <25 years old: No screening required
- 21-29 years (sexually active): Pap smear every 3 years
- 30-65 years: HPV DNA test and pap smear every 5 years OR pap smear alone every 3 years
- >65 years: no need screening if previous pap smears all negative and not high risk for cervical cancer.
If Pap smear reveals abnormality, patient will proceed with HPV DNA typing and colposcopy test.
Patients who have hysterectomy (surgical removal of the womb/uterus and cervix) before can stop cervical cancer screening unless their cervix is not removed, they have a history of CIN2/3 and history of cervical cancer.
Women with atypical squamous cells of undetermined significance (ASCUS) found on Pap smear but a negative HPV test can be rescreened with (Pap smear and HPV test) in 5 years or with Pap smear alone in 3 years.
Treatment of cervical cancer
Cervical cancer treatment is dependent on the stage of the cancer. For early invasive cancer, surgery is the treatment of choice. For advance cancers, combination of chemotherapy and radiation therapy is the standard of care. For patients with stage 4 disease whereby the cancer has spread to distant organs, the treatment is mainly palliative, chemotherapy and radiation therapy is to relieve symptom rather than cure.
Surgery
Laparoscopic (key-hole surgery) minimally invasive surgery reduces hospitalization stay, bleeding, analgesic requirements post-surgery, improved cosmetic effect and earlier return to daily activities. Types of surgery are:
1. Simple hysterectomy: Removal of the uterus (womb) and cervix.
2. Radical hysterectomy: Removal of the womb, cervix, Vagina, surrounding tissues and draining lymphatics.
3. Fertility Sparing Surgery: only reserved for very early stages of cancer as it only removes the cervix and preserves the uterus (womb) for fertility purposes.
Cervical cancer treatment is dependent on the stage of the cancer. For early invasive cancer, surgery is the treatment of choice. For advance cancers, combination of chemotherapy and radiation therapy is the standard of care. For patients with stage 4 disease whereby the cancer has spread to distant organs, the treatment is mainly palliative, chemotherapy and radiation therapy is to relieve symptom rather than cure.
Surgery
Laparoscopic (key-hole surgery) minimally invasive surgery reduces hospitalization stay, bleeding, analgesic requirements post-surgery, improved cosmetic effect and earlier return to daily activities. Types of surgery are:
1. Simple hysterectomy: Removal of the uterus (womb) and cervix.
2. Radical hysterectomy: Removal of the womb, cervix, Vagina, surrounding tissues and draining lymphatics.
3. Fertility Sparing Surgery: only reserved for very early stages of cancer as it only removes the cervix and preserves the uterus (womb) for fertility purposes.
Different stages have different treatment:
1. Stage 0 (carcinoma in situ): Treated with surgery local ablative or excisional measures such as cryosurgery, laser ablation, and loop excision.
2. Stage 1A1: Treatment of choice is surgery i.e. Total hysterectomy, radical hysterectomy and conization.
3. Stage IA2, IB, or IIA: Treatment is either combined external beam radiation with brachytherapy (insertion of radioactive implants directly into the tissue) OR Radical hysterectomy with bilateral pelvic lymphadenectomy.
4. Stage IIB, III, or IVA cancer: chemotherapy in combination with radiation is the standard of care.
5. Stage IVB and recurrent cancer: Treatment is mainly palliative. Radiation therapy can control of bleeding and pain and chemotherapy is for disseminated disease. Recurrence of cancer post-surgery can be treated with chemotherapy and radiation therapy.
1. Stage 0 (carcinoma in situ): Treated with surgery local ablative or excisional measures such as cryosurgery, laser ablation, and loop excision.
2. Stage 1A1: Treatment of choice is surgery i.e. Total hysterectomy, radical hysterectomy and conization.
3. Stage IA2, IB, or IIA: Treatment is either combined external beam radiation with brachytherapy (insertion of radioactive implants directly into the tissue) OR Radical hysterectomy with bilateral pelvic lymphadenectomy.
4. Stage IIB, III, or IVA cancer: chemotherapy in combination with radiation is the standard of care.
5. Stage IVB and recurrent cancer: Treatment is mainly palliative. Radiation therapy can control of bleeding and pain and chemotherapy is for disseminated disease. Recurrence of cancer post-surgery can be treated with chemotherapy and radiation therapy.
Radiation therapy
Radiation therapy uses high energy x-ray beams to destroy the cancer cells. Radiation can be used externally via external beams or internally via radioactive implants. Acute side effects include gastrointestinal (GI) effects such as diarrhea, abdominal cramping, rectal discomfort, and bleeding. It can also cause cystitis (inflammation of bladder) and urinary tract infection.
Late adverse effects of radiation therapy usually appear 1-4 years after treatment. These include rectal or vaginal stenosis (narrowing), malabsorption, small bowel obstruction, radiation enteritis (intestine inflammation) and chronic cystitis (inflammation of bladder).
Radiation therapy uses high energy x-ray beams to destroy the cancer cells. Radiation can be used externally via external beams or internally via radioactive implants. Acute side effects include gastrointestinal (GI) effects such as diarrhea, abdominal cramping, rectal discomfort, and bleeding. It can also cause cystitis (inflammation of bladder) and urinary tract infection.
Late adverse effects of radiation therapy usually appear 1-4 years after treatment. These include rectal or vaginal stenosis (narrowing), malabsorption, small bowel obstruction, radiation enteritis (intestine inflammation) and chronic cystitis (inflammation of bladder).
Chemotherapy
Chemotherapy use of anti-cancer drugs to destroy cancer cells. Healthy growing cells can also be destroyed in the process. It can be given orally or intravenously. Side effects include gastrointestinal side effects (nausea, vomiting and diarrhea), hair loss, marrow suppression and opportunistic infections.
Chemotherapy use of anti-cancer drugs to destroy cancer cells. Healthy growing cells can also be destroyed in the process. It can be given orally or intravenously. Side effects include gastrointestinal side effects (nausea, vomiting and diarrhea), hair loss, marrow suppression and opportunistic infections.
Follow up
After treatment of cervical cancer, the patients should be followed up periodically to look out for recurrence of the disease.
After treatment of cervical cancer, the patients should be followed up periodically to look out for recurrence of the disease.
