
What is vaginal cancer?
Vaginal cancer refers to the cancer of the vagina. Vagina is the birth canal, a muscular tube that connects the womb (uterus) to the outer genitalia area. Primary cancer of vagina originates from the cells that line the surface of vagina. It is very rare. Secondary cancer of vagina is more common and occurs as a result spread of cancer from adjacent structures e.g. cervix or uterus.
Vaginal cancer refers to the cancer of the vagina. Vagina is the birth canal, a muscular tube that connects the womb (uterus) to the outer genitalia area. Primary cancer of vagina originates from the cells that line the surface of vagina. It is very rare. Secondary cancer of vagina is more common and occurs as a result spread of cancer from adjacent structures e.g. cervix or uterus.
Types of Vaginal Cancer
The vaginal cancer can derive from different cells and hence form different types of vaginal cancer.
1.Squamous cell carcinoma: begins in the squamous cells (thin, flat cells) that line the surface of the vagina. It is most common form of vaginal cancer. It affects woman around 50-70 years.
2.Adenocarcinoma: begins in the glandular cells on the surface of vagina. It affects younger women as young as less than 25 years old.
3.Melanoma: begins in the melanocytes (pigment-producing cells) of vagina
4.Sarcoma: begins in the connective tissue cells or muscles cells in the walls of vagina.
The vaginal cancer can derive from different cells and hence form different types of vaginal cancer.
1.Squamous cell carcinoma: begins in the squamous cells (thin, flat cells) that line the surface of the vagina. It is most common form of vaginal cancer. It affects woman around 50-70 years.
2.Adenocarcinoma: begins in the glandular cells on the surface of vagina. It affects younger women as young as less than 25 years old.
3.Melanoma: begins in the melanocytes (pigment-producing cells) of vagina
4.Sarcoma: begins in the connective tissue cells or muscles cells in the walls of vagina.
What causes vaginal cancer?
The exact cause of vaginal cancer is unknown. Generally cancer occurs when genetic mutation causes healthy normal cells to undergoes changes and form cancer cells. When cancer cells divide, multiply and grow they form a cancer mass. The cancer can spread to adjacent structures, lymphatic system and via blood stream to distant organs like bones, liver and lungs.
There are a variety of risk factors that are associated with the development of vaginal cancer:
1.HPV: a sexually transmitted disease that not only causes HPV warts, it also is associated with cancers like vaginal cancer. Subtypes 16 and 18 are highly associated with cancers.
The exact cause of vaginal cancer is unknown. Generally cancer occurs when genetic mutation causes healthy normal cells to undergoes changes and form cancer cells. When cancer cells divide, multiply and grow they form a cancer mass. The cancer can spread to adjacent structures, lymphatic system and via blood stream to distant organs like bones, liver and lungs.
There are a variety of risk factors that are associated with the development of vaginal cancer:
1.HPV: a sexually transmitted disease that not only causes HPV warts, it also is associated with cancers like vaginal cancer. Subtypes 16 and 18 are highly associated with cancers.
2. Vaginal intraepithelial neoplasia (VAIN): A pre-cancerous stage caused by HPV infection. The cells are abnormal and may develop into cancers but not all women with VAIN will eventually have vaginal cancer.
3. Age: increasing age increases the risk of cancer. Most cancers occur in women above 60 years old.
4. Diethylstilboestrol (DES): from 1938-1971, DES was prescribed as a miscarriage prevention drug. DES has been associated with development of clear cell adenocarcinoma in the women and daughters of women who took DES. It is especially associated with young girls in their teens and early 20s.
5.Vaginal Adenosis: It is a condition after DES exposure and causes abnormal cells to form in the vagina.
6.Smoking: doubles the risk of developing vaginal cancer.
7.Radiation therapy: to the pelvis is a risk factor for cancer.
8.History of gynecological cancer: Patient with history of cervical cancer is at higher risk of developing vaginal cancer.
3. Age: increasing age increases the risk of cancer. Most cancers occur in women above 60 years old.
4. Diethylstilboestrol (DES): from 1938-1971, DES was prescribed as a miscarriage prevention drug. DES has been associated with development of clear cell adenocarcinoma in the women and daughters of women who took DES. It is especially associated with young girls in their teens and early 20s.
5.Vaginal Adenosis: It is a condition after DES exposure and causes abnormal cells to form in the vagina.
6.Smoking: doubles the risk of developing vaginal cancer.
7.Radiation therapy: to the pelvis is a risk factor for cancer.
8.History of gynecological cancer: Patient with history of cervical cancer is at higher risk of developing vaginal cancer.
Clinical symptoms of vaginal cancer
In about 10-30% vaginal cancer patients may not present with any symptoms at all. Common symptoms are:
1.Vaginal bleeding: Most common symptom affecting about 65-80% of patients with vaginal cancer. Bleeding usually is not related to menses, it can occur after sex, post-menopause or in between menses.
2.Vaginal discharge: smelly or bloody discharge occurs in 30% of patients
3.Urinary symptoms: like dysuria (pain of urination), urgency, hematuria (blood in urine) and bladder pain occur in 20% of patients. It is caused by cancer invasion into the bladder region.
4.Pelvic pain: occur in 15-30% of patients.
5.Constipation: When cancer invade into the colon it can cause constipation and tenesmus (feeling of inadequate defecation).
6.Vaginal Mass/prolapse: in 10% of patients may present with vaginal mass/prolapse.
In about 10-30% vaginal cancer patients may not present with any symptoms at all. Common symptoms are:
1.Vaginal bleeding: Most common symptom affecting about 65-80% of patients with vaginal cancer. Bleeding usually is not related to menses, it can occur after sex, post-menopause or in between menses.
2.Vaginal discharge: smelly or bloody discharge occurs in 30% of patients
3.Urinary symptoms: like dysuria (pain of urination), urgency, hematuria (blood in urine) and bladder pain occur in 20% of patients. It is caused by cancer invasion into the bladder region.
4.Pelvic pain: occur in 15-30% of patients.
5.Constipation: When cancer invade into the colon it can cause constipation and tenesmus (feeling of inadequate defecation).
6.Vaginal Mass/prolapse: in 10% of patients may present with vaginal mass/prolapse.
Diagnosis of vaginal cancer
After taking a medical history from the patient, the gynecologist will go on and perform a physical examination. Pelvic examination will be conducted by gynecologists inserting 2 fingers into the vaginal and another hand over abdomen to palpate for mass, estimate size of uterus and position of ovaries.
After taking a medical history from the patient, the gynecologist will go on and perform a physical examination. Pelvic examination will be conducted by gynecologists inserting 2 fingers into the vaginal and another hand over abdomen to palpate for mass, estimate size of uterus and position of ovaries.
Next gynecologist will insert a speculum into the vaginal to visualize the vaginal walls and cervix to look for any suspicious cancerous mass.
At the same time, a pap smear will be done to collect cells from the cervix to send it to the laboratory to test for presence of cancerous cells.
If there is a suspicious lesion found, then colposcopy is performed. Colposcopy is a procedure whereby a colposcope (a lighted magnifying instrument) to examine the lesion at the vagina/cervix. Biopsy can be performed at same time whereby the abnormal tissue are taken from the vagina/cervix to be sent to the laboratory to look for presence of cancer cells.
Staging of vaginal cancer
Once the diagnosis of vaginal cancer has been made, staging of vaginal cancer will be done next. With the stages of vaginal cancer determined, it will aid the physician to determine the treatment plan for patient.
Staging can be done by further investigations and tests like:
1.Colposcopy and biopsy: As mentioned above, colposcopy is used to magnify and visualized the suspicious lesion. Biopsy is then done to determine the grade of cancer cells.
Once the diagnosis of vaginal cancer has been made, staging of vaginal cancer will be done next. With the stages of vaginal cancer determined, it will aid the physician to determine the treatment plan for patient.
Staging can be done by further investigations and tests like:
1.Colposcopy and biopsy: As mentioned above, colposcopy is used to magnify and visualized the suspicious lesion. Biopsy is then done to determine the grade of cancer cells.
2.Cystoscopy: is a procedure whereby the cystoscope (a thin tube like instrument with lens) is inserted into the bladder via the urethra to look for any spread of cancer into the bladder. If abnormal tissue is found, a biopsy will be done at same time.
3.Ureteroscopy: Ureteroscope is similar to cystoscope, is a tube like instrument with lens that is inserted from bladder up the ureter to look for any invasion of cancer. If abnormal tissue is found, a biopsy will be done at same time.
4.Proctoscopy: Proctoscope a tube like instrument with lens is inserted into the anus to examine the anus and rectum to look for any presence of cancer spread from vagina. If abnormal tissue is found, a biopsy will be done at same time.
5.Chest X-ray: To look for cancer spread to the lungs
6.CT Scan: A dye will be injected or a radio contrast is consumed and the patient goes through CT scan machine to allow imaging of the chest, abdomen and pelvis to look for any cancer spread from vagina to the other organs.
7.MRI scan: using magnetic resonance waves, multiple images are taken using the MRI machine to look for spread of cancer to distant organs similar to CT scan.
6.CT Scan: A dye will be injected or a radio contrast is consumed and the patient goes through CT scan machine to allow imaging of the chest, abdomen and pelvis to look for any cancer spread from vagina to the other organs.
7.MRI scan: using magnetic resonance waves, multiple images are taken using the MRI machine to look for spread of cancer to distant organs similar to CT scan.
8.Lymphangiogram: a procedure to x-ray the lymphatic system. A dye is inserted into the lymphatic system to light up the lymphatic drainage and look for any spread of cancer to the lymph nodes.
Stages of Vaginal Cancer
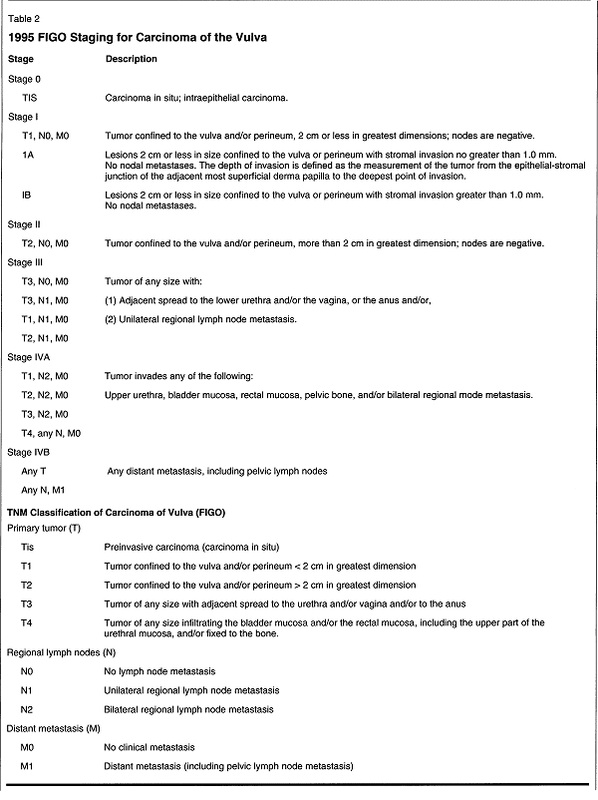
The stages of vaginal cancer range from stage 0 to 4 and is classified by the FIGO staging system as shown in table below:
The stages of vaginal cancer range from stage 0 to 4 and is classified by the FIGO staging system as shown in table below:
Treatment of Vaginal Cancer
The treatment of vaginal cancer is dependent on the stage of the disease, the location of the cancer, the size of the tumor, the type of vaginal cancer and also patient’s fitness for surgery.
Surgery is the commonest treatment plan. Other treatment modalities are radiation therapy and chemotherapy.
Surgery
Most vaginal cancer patients undergo surgery procedures if they are medically fit for operation. However if the vaginal cancer has spread widely to lymph nodes and multiple organs, surgery is not advised as it is no longer curative.
The types of surgical procedures include:
1.Laser Surgery: using laser as surgical blade to remove the tumor.
2.Wide local excision: surgery to remove the cancer and a margin of healthy cells.
3.Vaginectomy: surgical removal of part of and all of the vagina.
The treatment of vaginal cancer is dependent on the stage of the disease, the location of the cancer, the size of the tumor, the type of vaginal cancer and also patient’s fitness for surgery.
Surgery is the commonest treatment plan. Other treatment modalities are radiation therapy and chemotherapy.
Surgery
Most vaginal cancer patients undergo surgery procedures if they are medically fit for operation. However if the vaginal cancer has spread widely to lymph nodes and multiple organs, surgery is not advised as it is no longer curative.
The types of surgical procedures include:
1.Laser Surgery: using laser as surgical blade to remove the tumor.
2.Wide local excision: surgery to remove the cancer and a margin of healthy cells.
3.Vaginectomy: surgical removal of part of and all of the vagina.
4.Total hysterectomy: Surgical removal of the uterus and cervix either by key hole surgery (laparoscopic) or open surgery from the vagina or abdomen.
5.Lymphadenectomy: the lymph nodes are removed and sent to laboratory to examine for any cancer cells.
6. Pelvic exenteration: Extensive pelvic surgery to remove the vagina, cervix, uterus, ovaries, lymph nodes and part of the colon and bladder involved. In some cases, patients may have permanent stoma an outlet into the abdomen for urine and stools to flow out from the body.
6. Pelvic exenteration: Extensive pelvic surgery to remove the vagina, cervix, uterus, ovaries, lymph nodes and part of the colon and bladder involved. In some cases, patients may have permanent stoma an outlet into the abdomen for urine and stools to flow out from the body.
After surgery, skin grafting methods will be used to reconstruct the vagina. To make sure no remnant cancer cells remain, post-surgery radiation therapy will be done as adjuvant add-on therapy.
Possible surgical complications include infection, bleeding, anesthetic risks, pulmonary embolus, anastomotic leakage, fistulas and strictures.
Radiation therapy
Radiation therapy is a cancer treatment which uses high energy x-ray beams to kill cancer cells and prevent them from growing further. External radiation involves radiation machine directing beams from outside the body to target areas. Internal radiation (brachytherapy) uses radioactive devices inserted into vagina/surround tissues and intermittently release radiation on target sites. The devices is subsequently removed. Repeated radiotherapy sessions will be needed.
Radiation therapy
Radiation therapy is a cancer treatment which uses high energy x-ray beams to kill cancer cells and prevent them from growing further. External radiation involves radiation machine directing beams from outside the body to target areas. Internal radiation (brachytherapy) uses radioactive devices inserted into vagina/surround tissues and intermittently release radiation on target sites. The devices is subsequently removed. Repeated radiotherapy sessions will be needed.
Chemotherapy
Chemotherapy uses anti-cancer drugs which can be consumed or injected to kill the abnormal cells. In the process healthy cells may also be affected resulting in side effects. Chemotherapy is also a form of adjuvant therapy often combined with radiation therapy post-surgery.
Chemotherapy uses anti-cancer drugs which can be consumed or injected to kill the abnormal cells. In the process healthy cells may also be affected resulting in side effects. Chemotherapy is also a form of adjuvant therapy often combined with radiation therapy post-surgery.
Follow up
After surgery, patients should be followed up routinely with their gynecologists to look out for recurrence of cancer. Right after surgery, gynecologists will follow up patients more closely to check on wound healing, signs of complications, necrosis (dead tissue), and infection, conditions of stoma, quality of life, sexual issues and check for recurrence. They should also undergo a follow up plus a pap smear every 3-6 monthly for next 5 years after surgery.
After surgery, patients should be followed up routinely with their gynecologists to look out for recurrence of cancer. Right after surgery, gynecologists will follow up patients more closely to check on wound healing, signs of complications, necrosis (dead tissue), and infection, conditions of stoma, quality of life, sexual issues and check for recurrence. They should also undergo a follow up plus a pap smear every 3-6 monthly for next 5 years after surgery.
